
 ESPN’s recent documentary The Last Dance chronicles the story of Michael Jordan and the Chicago Bulls during the 1997-98 season as they competed for their sixth NBA championship. While Jordan’s status as the greatest of all time is debated by some, most observers of the game recognize him as uniquely talented and the dominant player of his era. Anyone familiar with Jordan’s story is aware of his fierce competitiveness and strong work ethic, not just during games but also at practices. Ongoing practice is accepted as an essential part of performance in sports, even for athletes who perform at the highest levels. In other contexts, the verb practice carries a different meaning and indicates simply that someone is performing responsibilities and tasks associated with a particular profession. In medical professions, successful completion of board exams demonstrates a minimal level of competency, and is not indicative of expert level performance. This article describes the principles of deliberate practice and suggests ways that their application can improve the skill of O&P clinicians at every experience level.
ESPN’s recent documentary The Last Dance chronicles the story of Michael Jordan and the Chicago Bulls during the 1997-98 season as they competed for their sixth NBA championship. While Jordan’s status as the greatest of all time is debated by some, most observers of the game recognize him as uniquely talented and the dominant player of his era. Anyone familiar with Jordan’s story is aware of his fierce competitiveness and strong work ethic, not just during games but also at practices. Ongoing practice is accepted as an essential part of performance in sports, even for athletes who perform at the highest levels. In other contexts, the verb practice carries a different meaning and indicates simply that someone is performing responsibilities and tasks associated with a particular profession. In medical professions, successful completion of board exams demonstrates a minimal level of competency, and is not indicative of expert level performance. This article describes the principles of deliberate practice and suggests ways that their application can improve the skill of O&P clinicians at every experience level.
Experience Is Not Expertise
Repeating an activity many times over a long period of time is not the same as acquiring expertise. (Many of us need look no further than our golf games for evidence of this.) The psychologist and researcher Anders Ericsson, PhD, has studied expert performance for decades and published hundreds of peer-reviewed papers on the topic.2 In 2016 he published Peak: Secrets from the New Science of Expertise, which is intended for a more general audience.3 According to Ericsson, “Nobody becomes an outstanding professional without experience, but extensive experience does not invariably lead people to become experts…. [Most] professionals reach a stable, average level of performance within a relatively short time frame and maintain this mediocre status for the rest of their careers.”4 When examining the cognitive mechanisms used by expert performers, Ericsson found “a complex structure that could not be accounted for by a mere accumulation of experience and knowledge.”5 Expert performance is achieved through continual improvement for many years after skills were initially acquired.
When preparing for a clinical role, the focus is on achieving a minimum level of competency, after which individuals transition from providing care with supervision to doing so independently. After the entry level of competence has been confirmed through a credentialing process, education and training is often focused on the introduction of new techniques, rather than the improvement of established skills. Most O&P students and residents recognize their skills require considerable improvement. It is less common for experienced clinicians to realize that “more experience does not, by itself, lead to improvements” in performance.5 Awareness of this phenomenon can motivate novice and experienced clinicians alike to evaluate their performance. Understanding how experts train and applying those principles can improve skills regardless of where individuals fall on the spectrum from entry level to expert.
Deliberate Practice Defined
While studying the performance of students of the violin, Ericsson observed that their training involved individualized practice under the guidance of skilled teachers who passed on what they learned in a uniform manner. Further research revealed principles and behaviors, which came to be known as deliberate practice, that contributed to improvement and expertise in many different disciplines, including medicine. Ericsson found that this type of practice was most effective in fields that involved objective criteria for assessing performance, a skilled teacher, and structured practice methods. Other traits of deliberate practice are listed in Figure 1. 
It can be challenging to apply deliberate practice methods to O&P clinical and technical practice, since there are few universally acknowledged, objective criteria that define success for clinical decision-making, assessment, and many other tasks we perform daily. There is no equivalent of a score board or statistics to measure and compare practitioner performance over time or differences in performance between practitioners. However, many clinical and technical tasks involve specific procedures that can be evaluated using the qualitative criteria that define the art of clinical practice and that we use on a daily basis to determine the quality of our performance.
Ericsson reports that improvements in performance occur when individuals are “1) given a task with a well-defined goal, 2) motivated to improve, 3) provided with feedback, and 4) provided with ample opportunities for repetition and gradual refinements of their performance.”5 These conditions either already exist in clinical practice or they can be created with minimal difficulty. While we lack definitive objective criteria for determining the quality of an impression or dynamic alignment, many complex activities can be broken down into discrete actions and decisions that can become the focus of improvement. An important aspect of skill development is the identification by an experienced clinician of “representative tasks that define the essence” of the associated tasks.4 Students rely completely on instructors to identify these tasks and the desired performance level. As experience increases, thoughtful practitioners can begin to identify distinct events amenable to improvement as well as what characteristics indicate improvement. According to Ericsson, “The distinctive aspect of the expert-performance approach to the study of expertise is its focus on identifying superior, reproducible behavior for representative tasks in the associated domain.”4 Observing how acknowledged experts manipulate tools and materials, position themselves and the patient, attend to visual cues, communicate with others, and many other specifics of a clinical encounter can become the focus of improvement. When using plaster bandage to take an impression, students may begin with a focus on avoiding gaps, roping, or other obvious errors. As skill increases, practitioners can focus on more aspects of the shape capture to achieve specific clinical goals.
The Importance of Feedback
An essential component of deliberate practice is the “detailed immediate feedback” provided by a more skilled teacher.4 For feedback to be valuable, the performance must be observed directly, the feedback must address specific actions that are the focus of improvement, it should be provided as soon as possible, and the learner must accept the feedback and modify his or her performance accordingly. The college basketball coach Dean Smith and Jordan’s batting coach when he was briefly a part of the White Sox organization many years later both observed his receptiveness to feedback.6 Perhaps more importantly, Jordan himself recognized this trait as crucial to his success: “My greatest skill was being teachable. I was like a sponge. Even if I thought my coaches were wrong, I tried to listen and learn something.”6
Clinicians at every skill level benefit from not only accepting feedback but actively seeking it out. Experienced practitioners may forget that tasks they consider routine can be overwhelming to someone with less experience. Limiting the number and length of training encounters to allow sufficient time and energy for discussions about performance will facilitate the learning process. Ericsson’s observation applies to all learners: “The best training situations focus on activities of short duration with opportunities for immediate feedback, reflection, and corrections.”5 A busy clinical practice provides many opportunities to use repeated patient encounters to focus on specific skills. Taking time to reflect on the performance during and immediately following each encounter contributes more to skill development than simply repeating a task multiple times. General requests for feedback usually result in general, and less useful, feedback. One way to facilitate the feedback process is for learners to ask for one or two specific ways that they can improve their performance in a task. Asking “What is one thing I can do to wrap plaster more smoothly?” will result in more meaningful feedback than asking “How did I do on this impression?”
The Danger of Being Automatic
Once a basic level of competence has been achieved, performance in many clinical tasks may not require much focus or attention. Experienced clinicians can perform tasks intuitively, responding instinctively to situations by doing what has achieved adequate results in the past. This approach has several drawbacks. First, intuitive performance cannot be taught explicitly. A practitioner relying on intuition when performing a process has little to offer a student or trainee who has not yet developed the core skills required to perform the task at a more basic level. One of the characteristics that defines expert performers is that they “are able to report their thought processes and critical aspects of the encountered situations.”5 This ability to describe the rationale behind decisions and actions is required both to progress toward expert performance and to be an effective teacher. Secondly, while automatic performance may suffice for routine tasks, it does not prepare clinicians effectively for challenging or exceptional cases. In more difficult situations, clinicians need to apply prior expertise to a new, more challenging situation, and this requires an explicit awareness of the factors that are likely to result in a successful outcome.
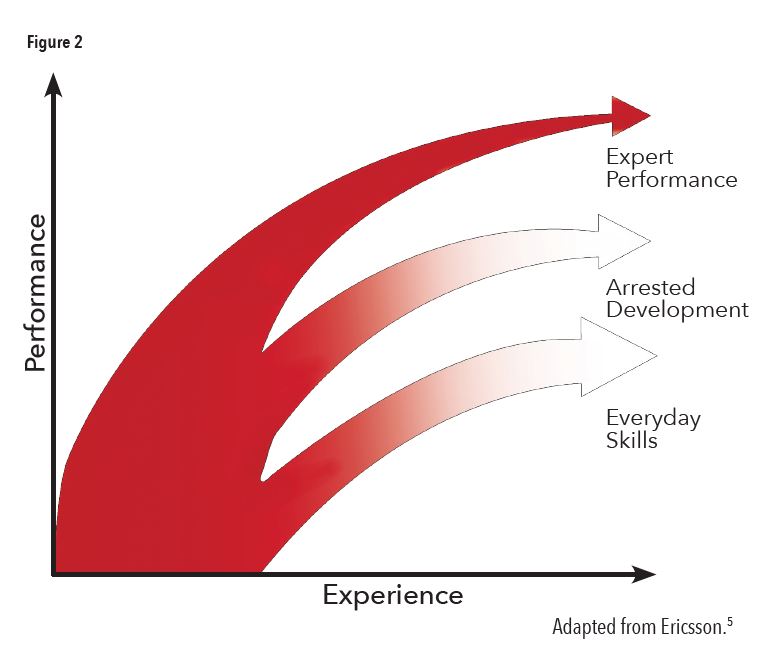
A third drawback of intuitive practice is that it does not result in improvement. “When performance has reached this level of automaticity and effortless execution, additional experience will not improve the accuracy of behavior nor refine the structure of the mediating mechanisms, and consequently, the amount of accumulated experience will not be related to higher levels of performance.”5 As shown in Figure 2, skill development is arrested when the performance becomes automatic. Skills will only continue to improve if clinicians employ the same approach to learning that they did at the beginning of their careers. Experts “counteract tendencies toward automaticity by actively setting new goals and higher performance standards, which require them to increase speed, accuracy, and control over their actions…” and “deliberately construct and seek out training situations to attain desired goals that exceed their current level of reliable performance.”5
I once spoke with an owner of an O&P central fabrication facility who described reaching a point in his career as a technician when he was no longer challenged by daily technical tasks. To remain engaged with his work, he began timing how long it took to complete tasks and worked purposefully to complete them in less time while maintaining quality. Not only did this positively impact his employer, but according to principles described by Ericsson, it also put him on the path to becoming an expert.
Is maintaining the same skill level problematic, as long as the tasks are performed at an acceptable level? In other words, why is good enough not good enough? There is evidence that without deliberate practice some skills actually decline over time. Ericsson describes a 1960 study involving the diagnosis of heart sounds of healthy and ill patients by medical students and physicians. As expected, the accuracy of diagnosis by students and residents increased in response to their training and was highest among specialists (cardiologists). However, the diagnostic accuracy of general practice physicians actually declined the further removed they were from the end of their training.4 It is the purposeful practice of a procedure, rather than simply performing it repeatedly, that improves skill: “Tennis players will not improve their backhand volley in tennis by playing more games.”4
Closing Thoughts
Few of us will become as well known for our skills as Michael Jordan has been for his. However, any improvement in our clinical abilities benefits our patients. Identifying specific clinical and technical skills that we would like to improve upon, focusing our attention and effort in those areas, and actively soliciting feedback from others can all contribute to this important goal.
John T. Brinkmann, MA, CPO/L, FAAOP(D), is an assistant professor at Northwestern University Prosthetics-Orthotics Center. He has over 25 years of experience in patient care and education.
References
1. Scheidies, N. 2020. How to Be Like Mike: 21 Life Lessons from Michael Jordan. IncomeDiary. https://www.incomediary.com/how-to-be-like-mike-20-life-lessons-from-michael-jordan
2. https://scholar.google.com/citations?hl=en&user=Ym0clGUAAAAJ&view_op=list_works&sortby=pubdate
3. Ericsson, A., and R. Pool. 2016. Peak: Secrets from the New Science of Expertise. Houghton Mifflin Harcourt.
4. Ericsson, K. A. 2004. Deliberate practice and the acquisition and maintenance of expert performance in medicine and related domains. Academic Medicine 79(10):S70-81.
5. Ericsson, K. A. 2008. Deliberate practice and acquisition of expert performance: a general overview. Academic Emergency Medicine 15(11):988-94.
6. Lazenby, R. 2014. Michael Jordan: The life. Little, Brown and Company.
Support authors and subscribe to content
This is premium stuff. Subscribe to read the entire article.

