
Controlling excessive foot pronation is an important aspect of managing many lower-limb pathologies such as plantar fasciitis, posterior tibial tendon dysfunction, pediatric flexible flatfoot, and medial tibial stress syndrome. Supporting the medial longitudinal arch of the foot with orthotics helps position it to improve its function and alleviate symptoms of lower-limb pain.
The medial heel skive technique, also known as the Kirby skive, is a modification that has proven effective for improving pronation control. Developed by Kevin Kirby, DPM, MS, in the early 1990s, this method of cast modification enhances force dynamics at the heel to exert greater influence on subtalar joint motion.1 It is effective in individuals with excessive pronation and especially those with a medially deviated subtalar joint axis (STJA). 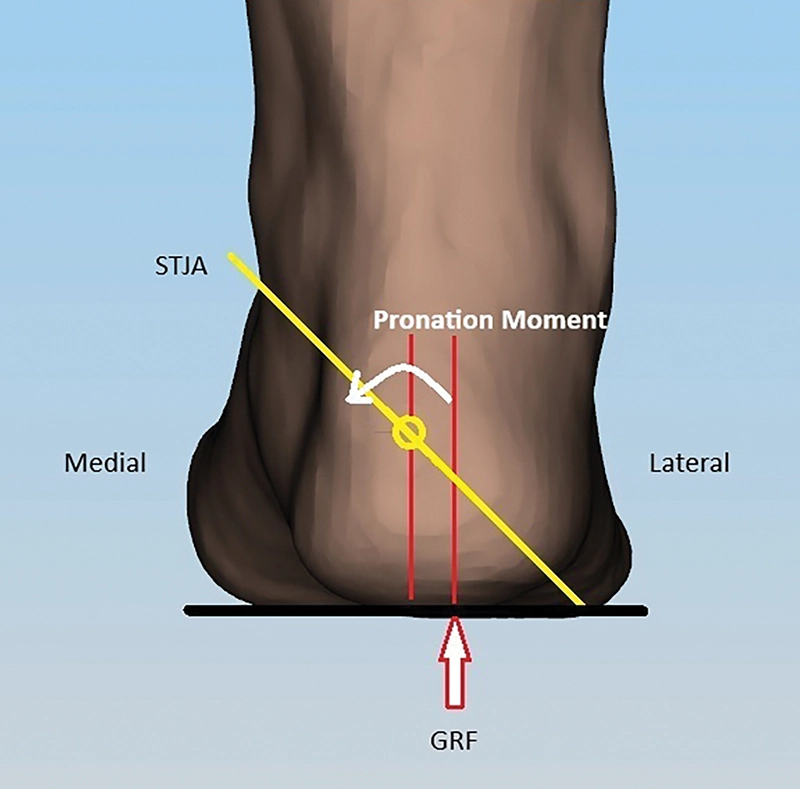
Support authors and subscribe to content
This is premium stuff. Subscribe to read the entire article.


{kind=link}