
 I remember feeling overwhelmed when I treated my first patient who had a hip disarticulation. I imagine that would be a common reaction for a practitioner who does not see that level of amputation often. I hope this article will provide more knowledge to address hip disarticulation and help practitioners feel more confident when treating a patient with this type of amputation.
I remember feeling overwhelmed when I treated my first patient who had a hip disarticulation. I imagine that would be a common reaction for a practitioner who does not see that level of amputation often. I hope this article will provide more knowledge to address hip disarticulation and help practitioners feel more confident when treating a patient with this type of amputation.
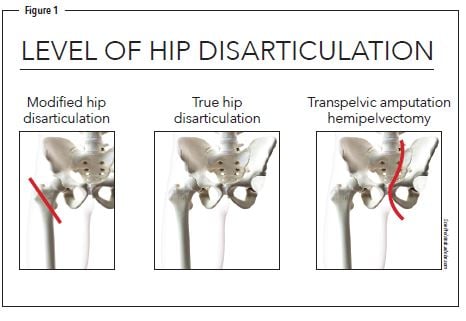
Hip disarticulation is a complex and infrequent surgery, which involves either leaving a very small portion of the femur or separating the ball from the socket of the hip joint (Figure 1). It accounts for 0.5 to 2 percent of lower-limb amputations and is only performed as the last option in extreme cases. The most common cause of this amputation level is a highly invasive tumor that is unresectable, with limb ischemia, trauma, and severe musculoskeletal infections of the pelvic region as additional etiologies.1
This presentation is so rare that many practitioners will never have a case in their careers. For those who do, traditional treatments historically did not offer the best outcomes. Much of the literature shows many patients abandon their prosthesis if they find it too uncomfortable or difficult to use.
The traditional prosthetic solution we were taught in school, often referred to as the Canadian design, included strapping a bulky bucket-like socket to the patient, which can be heavy and uncomfortable to ambulate with or sit. Over time, material sciences have improved, so we can make the sockets lighter weight and more comfortable for those needing a more traditional fit.
Another problem practitioners face is the level of expectation sometimes set by the treating physician. People with amputations at this level are often told they will require an assistive device such as a wheelchair, walker, or crutches and not informed there may be a prosthetic option. Many physicians are not aware of the newer technology, socket designs, and components that are available.2
The way to better outcomes for this population are comfortable sockets and appropriate prosthetic componentry and technology to help patients minimize their energy expenditure.
The Progression of Socket Designs
Getting a comfortable socket fit is one of the most difficult and imperative parts of the process. It almost seems to be a contradiction with socket fits: The socket has to be tight and secure so it does not slip, but also flexibleenough to be comfortable when sitting and ambulating. This can be compounded by the presentation of the residual limb. Surgeons are often focused on saving the patient’s life and not future prosthetic use.
To understand socket comfort, let’s look at some previous and current sockets designs. In the 1940s, the socket consisted of molded leather with a laterally placed hip joint called a tilting table prosthesis. In 1954, the Canadian design was introduced by McLaurin, which is commonly a standard of socket fit with a free hip, knee, and ankle joint. The saucer-type prosthesis was introduced for people with very short transfemoral amputations because adequate stability could not be achieved without the additional bone support (Figure 2).
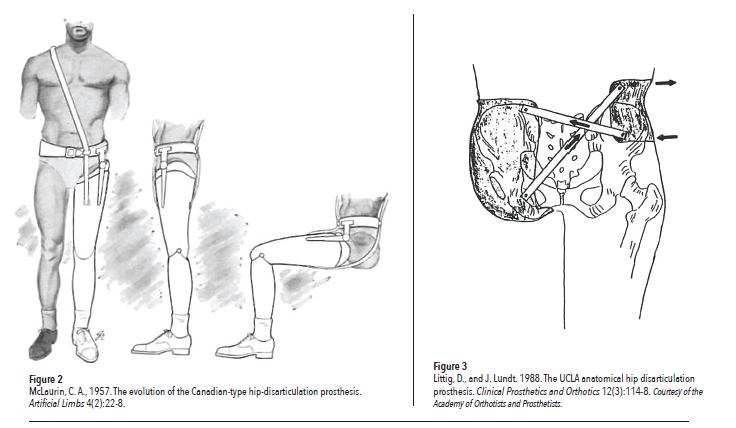
In 1980, the University of California Los Angeles introduced the anatomical hip disarticulation socket (Figure 3). This design encapsulates the ischium and ischial ramus to provide more comfort and to detail the ischial ramus angle and the medial inclination of the ischium.
In early 1990s, Dycor’s Roller Track socket was introduced (Figure 4). This design positioned the hip joint in the center of the socket rather than anteriorly in hopes of achieving better toe clearance during swing. This design also used a laterally mounted hip joint.
Another treatment that became available in 2000, the silicone frame socket, is an ischial ramus containment and fastens the pelvis diagonally on both sides between the iliac crest and ischial tuberosity. This is definitely one of the lighter weight systems used for fabricating a hip disarticulation prosthesis. I’ve tried a modified version of this with mild success. We tried using prepreg and our technician made a silicone inner socket.
Clinicians began using the Glenrose semi-flexible socket, which reduces the amount of material used as a stabilizing force and uses more flexible materials, in 2005. It utilizes three layers and a unique contralateral anchor design around the iliac crest. It is sometimes referred to as the butterfly system. It uses diagonally medial/lateral forces to help reduce the anterior/posterior forces usually used to drive the prosthesis.
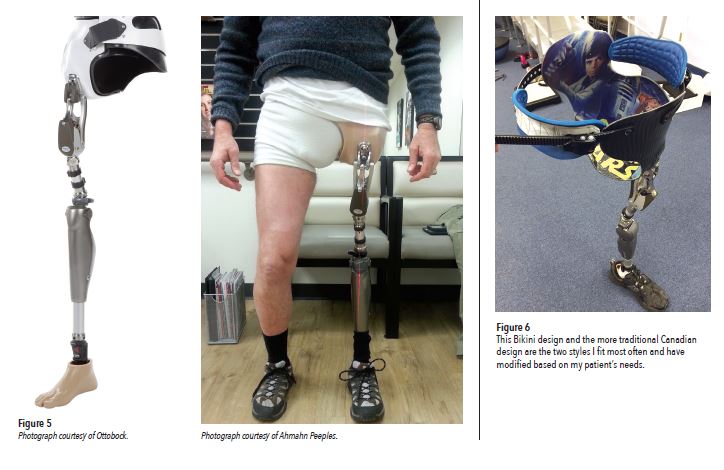
The most recent take on hip sockets is the Bikini Socket developed by Jay Martin, CP, FAAOP, in 2013. This system uses two floating iliac crest stabilizers without encapsulating the entire pelvis to provide more direct biomechanical link between device and user.
Component Options
Many of the hip joints are single axis with or without extension assist and a manual lock. As with any modular component, as the patient’s activity level increases, so should the capability of components to support it. There is also the polycentric joint option. This is most recently available as a hydraulic unit. With this upgrade, we can now help with controlling pelvis tilt and extension of the device in multiple phases of gait because of the joint’s dampening capability. One other hip joint is the Helix 3D (Figure 5). The three-dimensional aspect of this joint is the relationship between the hip joint extension/flexion and transverse rotation. This is the most advanced hip joint on the market to help with increased stability, mobility, and comfort.
Next in the line of progression is the prosthetic knee. For this high-level amputation, I would consider using polycentric knee units, with or without fluid control. They may be little heavier, but the tradeoff is increased stance phase stability. Because of the multi-linkage design, the knee does not erode as the knee mechanism wears with time, increased cadence is possible, and there is separate adjustability of extension and flexion resistance. Another knee to consider is a microprocessor-controlled knee. This allows the patient to have better control on variable terrains, helps reduce risk for falls, reduces conscious effort of walking, and offers adjustable extension and flexion resistance.
The final component to address is the foot/ankle complex. Dynamic response feet are commonly used because they are light weight and have multi-axial properties for patients to walk on uneven terrain. For less active patients, SACH feet or single axis feet can also be a consideration.
It is important to have several angled adapters readily available to help establish the connection between the pyramid adapter of the knee and the pylon of the anterior mounted hip joint.
Alignment and Force Considerations
At initial contact, heel strike, the ground force reaction (GRF) passes posterior to the ankle axis, the heel is compressed, and the foot is lowered to the ground. At the same time an extension moment is created at the knee as the GRF passes anterior to the knee joint. By midstance, the GRF passes posterior the hip joint and anterior to the knee joint. With forward progression into pre-swing, the GRF moves posterior to the knee, allowing the knee to bend and facilitate swing phase of the foot for clearance, while weight is shifted to the opposite limb.
Part two of this article will review more biomechanics, alignment, and casting techniques for this population.
Ahmahn Peeples, LCPO, ACSM-CPT, EIM, is a clinician with more than 15 years of experience in patient care and education. He is a staff clinician and Outcomes Southwest Regional Champion with Hanger Clinic. He can be contacted at apeeples@hanger.com.
References
Dillingham, T. R, L. E. Pezzin, and E. J. MacKenzie. 2002. Limb amputation and limb deficiency: epidemiology and recent trends in the United States. Southern Medical Journal 95(8):875-83.
Endean, E. D., T.H. Schwarcz, D.E. Barker, N.A. Munfakh, R. Wilson-Neely, and G.L. Hyde. 1991.
Hip disarticulation: Factors affecting outcomes. Journal of Vascular Surgery 14 (3) 398-404.




{kind=link}