
Urgent concern regarding diabetes is not only a health issue in the United States but it is a global epidemic easily affecting half a billion people. A host of factors from less active lifestyles, diets high in sugar and refined foods, and a general trend towards obesity has led to a dramatic increase in the diagnosis of type 2 diabetes. Among its many long-term effects, diabetes leads to peripheral neuropathy, making the foot susceptible to ulceration. Diabetes is the pathway for the majority of non-traumatic lower-limb amputations in the United States. According to statistics from the World Health Organization, diabetes mellitus is the seventh leading cause of death globally.
Management of the Diabetic Foot
Since the mid-1990s, the International Working Group on the Diabetic Foot (IWGDF) has published evidence-based guidelines on the prevention and management of diabetic foot disease. Their reports, seven in all, include updated guidelines based on current research from studies and meta-analyses. They employ well-established methodologies to conduct systematic reviews of the most recent literature and from that develop recommendations for off-loading and preventing diabetic foot ulcers and amputations.
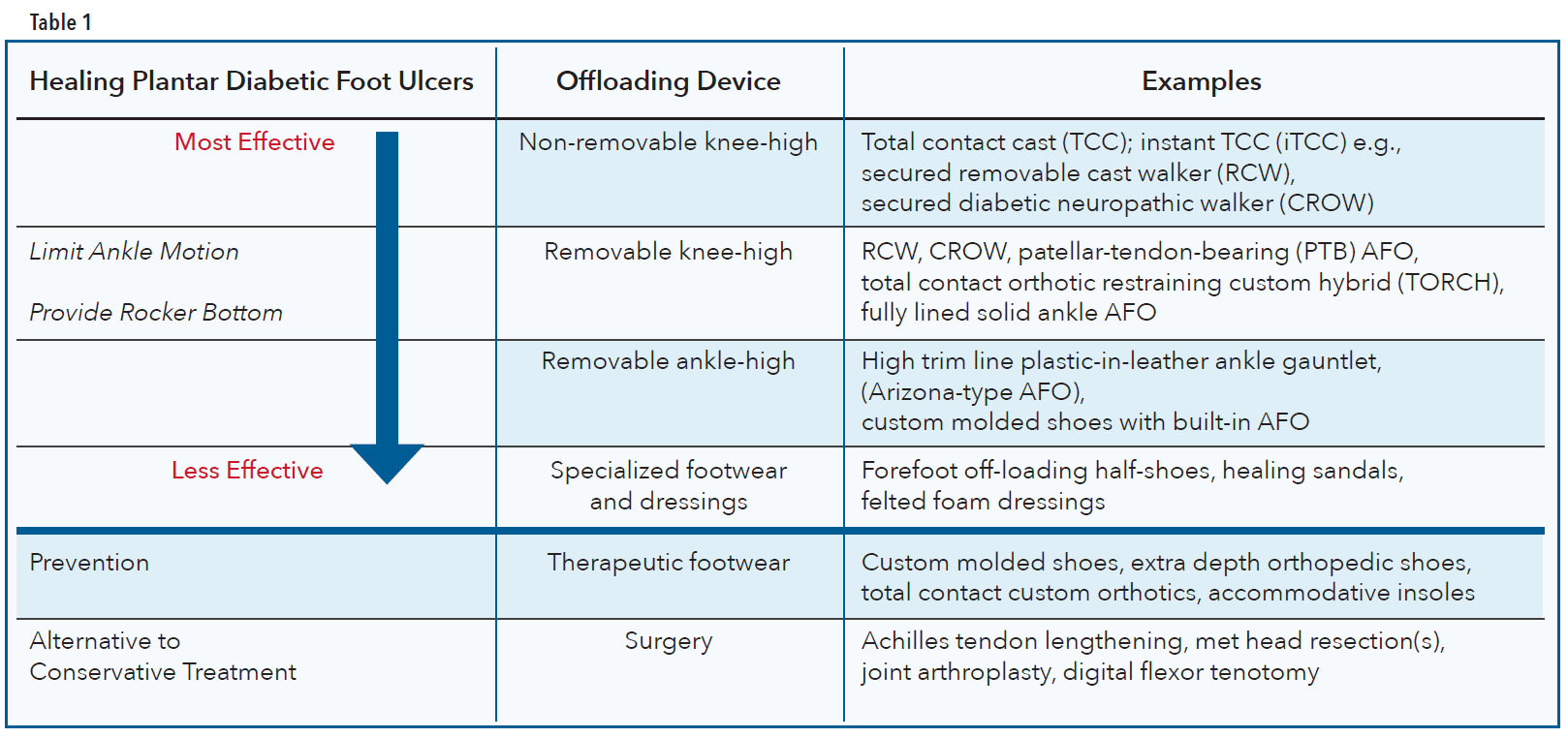
Their recommendations for healing a neuropathic plantar forefoot or midfoot ulcer in a person with diabetes can be summarized in several choices of treatment (Table 1). The first choice of treatment is a nonremovable knee-high offloading device. This should incorporate an appropriate foot-device interface to alleviate and redistribute pressure. If contraindications such as infection, ischemia, or patient intolerance to nonremovable devices exists, then removable knee-high and removable ankle-high off-loading devices are to be considered as the second and third choice off-loading treatment, respectively. Appropriately fitting footwear combined with felted foam is the fourth choice but should only be considered when none of the previous options are possible. If these nonsurgical, conservative off-loading approaches fail, only then should surgical interventions be considered for healing metatarsal head and digital ulcers. There are other specific guidelines for cases when infection or ischemia are present.
Patients with plantar heel ulcers should also consider using knee-high off-loading devices or other interventions to reduce plantar pressure on the heel. Finally, to heal nonplantar foot ulcers it is recommended to use ankle-high devices, footwear modifications, toe spacers, or orthotics.
Biomechanics of Breakdown
Although diabetes is a metabolic disease, the development of a plantar foot ulcer can be considered biomechanical in nature. In normal gait the heel contacts the ground first and as gait progresses the body passes over the plantigrade foot. The stance leg and foot accept the full load of body weight as the contralateral limb goes through swing. One of the requirements for smooth and asymptomatic ambulation is fluid and free joint motion, especially at the ankle and first metatarsophalangeal joint (MPJ).
One of the side effects of diabetes and uncontrolled blood sugars is the process of glycosylation, an irreversible cross-linking of collagen and keratin. This causes a thickening of the skin, tendons, ligaments, and joint capsules. It leads to a reduction in joint flexibility and motion, termed limited joint mobility (LJM), leaving the tissue compromised. If, as a result of glycosylation, the necessary ankle dorsiflexion is not available, there will be higher continuous pressure on the forefoot through the midstance and propulsive phases. Likewise, any restriction of motion at the first MPJ alters gait and elevates pressure beneath the hallux. These increased pressures due to LJM, in conjunction with peripheral neuropathy, are closely related with higher incidences of forefoot ulceration.
Over time, people with diabetes may also experience some level of muscle atrophy that deforms the toes and feet and encourages anterior migration of the plantar fat pads. These musculoskeletal changes result in midfoot bony prominences, dropped metatarsal heads, and hammertoes, which become focal sites for pressure and shear, leading to calluses on the skin. As it is established that the presence of a plantar callus is highly predictive of ulceration, inspecting for and preventing calluses is a known way to avoid ulceration.
Recommended Devices
Any AFO or mechanical intervention that limits ankle motion, keeping the foot at 90 degrees to the leg, will help reduce loading on the midfoot and forefoot later in the gait cycle. The shortened stride length and decreased cadence help reduce the intensity of repetitive cycling. As an aid to ambulation, many rigid-ankle devices are made with rockers or controlled ankle motion (CAM) soles to smooth out the step. One caution with any of these orthoses is that they may lose effectiveness if edema subsides.

Solid Ankle AFO, Plastazote lined

CROW

PTB Crow

Support authors and subscribe to content
This is premium stuff. Subscribe to read the entire article.


