
The details of my first experience independently providing orthotic services in an operating room are etched indelibly in my memory. The case involved a patient who required a knee orthosis immediately following total knee arthroplasty. I was directed to a spot in the corner where I could wait unobtrusively and be available to fit the orthosis when the surgery was finished. Being too far away to observe the procedure and only able to make out snippets of the conversation occurring at the operating table, my mind began to drift to other matters. My reverie was interrupted abruptly when I realized that the surgeon had asked about the patient’s pre-operative range of motion (ROM) and all eyes in the room were focused on me. The surgeon repeated the question more firmly. I said that I had not seen the patient before and didn’t know the ROM. I vividly remember the impatience and anger in the surgeon’s voice when he shouted: “Look in the chart!”
I then realized that the patient’s paper chart was on a small shelf just below the x-ray viewing box I was standing next to. I flipped frantically through the pages looking for what I assumed would be detailed ROM information. The relief I felt when I found the pre-operative note quickly turned to panic when I read: “Patient’s knee is messed up—needs to be replaced.” When I stammered something along the lines of not being able to find specific numbers, the surgeon let out a disgusted sigh and diverted his attention back the patient’s limb.
I shrunk back into the corner with the distinct feeling that I’d failed in a significant way. My rumination was interrupted a few minutes later by another outburst from the surgeon, this time followed by the sharp clattering noise as the instrument he’d thrown skittered across the floor and into the wall. It did not appear that the instrument had been aimed at anyone, but I decided to pay closer attention in case any objects came hurtling in my direction.
This article summarizes two systematic reviews related to how unacceptable and disruptive behavior impacts team dynamics and patient care. Gou et al. reviewed 36 studies to determine “the published evidence on the impact of exposure to unacceptable behavior between HCWs [healthcare workers] on clinical performance” and “whether exposure to unacceptable behavior affects quality of care, workplace productivity, and patient outcomes.”1 Hicks and Stavropoulou reviewed 25 studies “to identify and synthesize the empirical evidence on the effect of HCP DB [healthcare professional disruptive behavior] on at least one of the following outcome measures of patient care: clinical outcomes, patient safety, patient satisfaction, or quality of care.”2
Types of Disruptive Behavior
A variety of terms and definitions are used in medical literature to describe inappropriate behavior. Gou et al. described unacceptable behavior as “negative behavior that violates the norms for mutual respect, and includes rude, dismissive, aggressive, and discourteous behavior” and identified “bullying, discrimination, and harassment” as behaviors that are “legislated or reflected in nonregulatory instruments in several countries….”1 They reported that “the word ‘incivility’ has been used extensively in the medical literature to describe unacceptable behavior,” and stated that this term “has a difficult history, particularly for people from racial and ethnic minorities, as it evokes memories of their struggle for equity.”1 Hicks and Stavropoulou described disruptive behavior as “an umbrella term that captures any inappropriate behavior by HCPs that has the potential to undermine a culture of safety or jeopardize quality healthcare delivery.”2 This includes “a variety of behaviors or confrontations ranging from noncollaboration and verbal abuse to physical or sexual harassment. Disruptive behavior includes but is not limited to bullying, incivility, and horizontal/lateral violence.”2
Gou et al. pointed out that “while most definitions of workplace bullying require that the behavior is frequent and has clear intention of harming the target, unacceptable behavior also encompasses behavior with (1) unclear or ambiguous intent to harm, (2) low intensity, and (3) low frequency as the effects of these behaviors are independent of the frequency of exposure.”1 This is supported by Hicks and Stavropoulou, who reported that “persistent, low-level behaviors that are often normalized in everyday clinical settings are just as harmful as the higher-intensity behaviors.”2
During another exchange with the surgeon mentioned previously, he exhibited lower-level disruptive behavior. I happened to see him walking down the hallway of the hospital and took the opportunity to talk with him about a patient he had referred for orthotic care. I matched his pace as he strode down the hall, introduced myself, and asked a question about the case. During the brief interaction, he never made eye contact or slowed his pace and gave no other indication that he considered my questions important. His curt responses made it clear that it was up to me to resolve the situation. While not as egregious as his actions in the operating room, his rude and dismissive behavior did not positively impact our relationship or the care provided to the patient.
Source and Frequency of Disruptive Behavior
It may be easy to assume that physicians are more often the perpetrators and lower-ranking HCPs more often the victims of disruptive behavior. Eighty percent of the 36 studies that Guo et al. reviewed involved nurses, 41 percent involved physicians, 11 percent involved nursing assistants and care aids, and only 5.5 percent involved allied health. These authors also reported that a systematic review of disruptive behavior (DB) in surgical workplaces found that “high rates of bullying and undermining behavior were…experienced by nurses, allied health staff, medical students, and doctors worldwide.”1 They reported that “in a 2015 survey of 606 doctors across three teaching hospitals in England, 31 percent of doctors described being subject to rude, dismissive, or aggressive behavior a few times a week or more, with junior doctors and registrars being twice as affected as consultants.”1 (Consultants are the highest ranking physicians in the British healthcare system, and registrars are physicians in specialty training.)
This supports assumptions about a relationship between HCP rank and DB. It is worth noting, however, that Hick and Stavropoulou’s systematic review found that “studies that reported DB among different professional groups saw an equal number of studies reporting a higher prevalence of DB among nonphysician groups and physician groups.”2 It is difficult to accurately determine the scale of the problem, since “underreporting of DB was a recurring theme” in the studies reviewed by Hicks et al., “with study participants reporting fear of identification, despite guarantees of confidentiality.”2 These authors go on to state that “the evidence suggests that most healthcare settings have normalized a low-level culture of DB in which HCPs have come to accept rude and aggressive behaviors as inevitable and justified by the stressful nature of the job. Disruptive behavior is considered a rite of passage into seniority.”2
How Unacceptable Behavior Disrupts
 Rudeness may seem like a relatively minor issue, but it detrimentally affects performance. Guo et al. described how rudeness “serves as a signal that there is a problem in the environment. As a result, cognitive resources are reallocated from task completion to situational processing….”1 They also reported that it “produces a state of physiological arousal, narrowing of perception, and more selective processing. This produces deficits in creative problem-solving, comprehension, and recall of prior knowledge.”2 Importantly, these negative effects impact the task performance not only of those who are objects of the behavior, but those who witness it.1
Rudeness may seem like a relatively minor issue, but it detrimentally affects performance. Guo et al. described how rudeness “serves as a signal that there is a problem in the environment. As a result, cognitive resources are reallocated from task completion to situational processing….”1 They also reported that it “produces a state of physiological arousal, narrowing of perception, and more selective processing. This produces deficits in creative problem-solving, comprehension, and recall of prior knowledge.”2 Importantly, these negative effects impact the task performance not only of those who are objects of the behavior, but those who witness it.1
I felt these physiological and cognitive effects in response to the surgeon’s behavior in both situations described above. It required additional conscious effort to refocus on the clinical problem rather than on the effects of his treatment of me and others on the team. According to Guo et al., “rudeness can incite retaliatory behavior or conscious effort to not allocate effort toward the required tasks, resulting in reduced helpfulness and impaired teamwork performance.”1 Perhaps one reason that disruptive behavior is often exhibited by higher ranking HCPs is that they assume those with lower rank are obliged to perform tasks and will do so regardless of how they are treated. O&P clinicians recognize their responsibility to act in the patient’s best interest, regardless of how they are treated or how they feel in response to that treatment. However, the subtle (or even unconscious) negative effects of disruptive behavior can lead to poorer performance and reduced quality of care.
 Negative Effects
Negative Effects
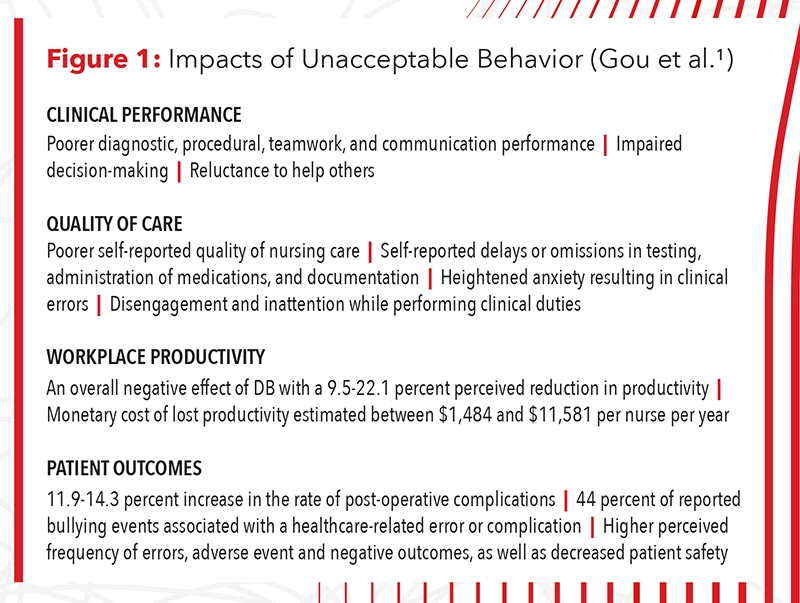
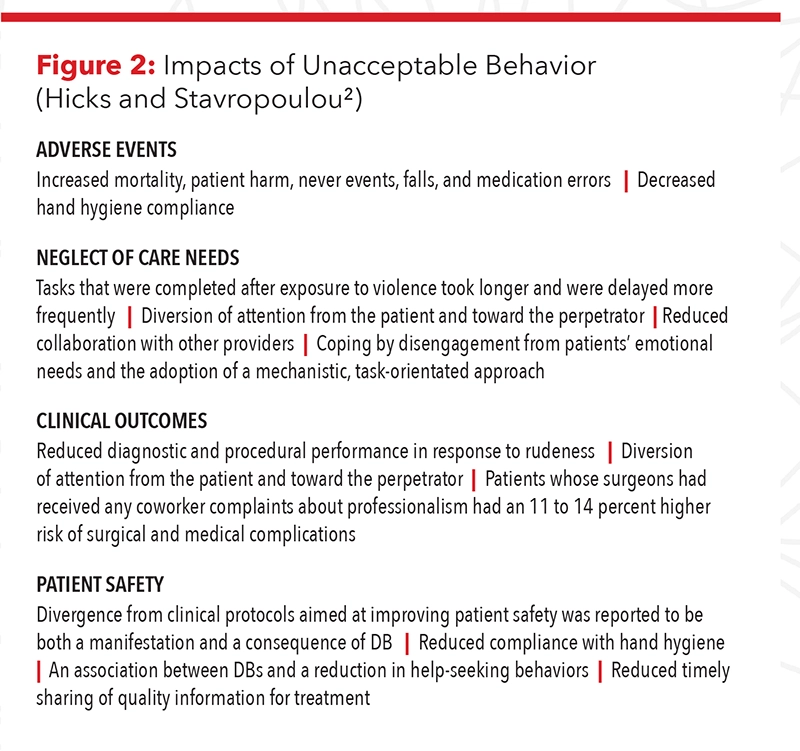
Guo et al. reported that “while there are some inconsistencies in the strength of the associations reported, the overall weight of evidence suggests that unacceptable behavior has widespread negative consequences with considerable implications for quality in healthcare delivery and patient safety. Of note, no study demonstrated beneficial effects from unacceptable behavior.”1 Hicks and Stavropoulou were more succinct in their conclusion that their review “shows that HCP DB negatively affects patient care.”2 A summary of the impacts of unacceptable behavior identified in the two studies can be found in Figures 1 and 2.
The two systematic reviews mentioned some interesting nuances. Guo et al. reported that “anesthesiology residents had significantly poorer performance when the simulated surgeon was portrayed as impatient, even without being overtly intimidating or using inappropriate language” and that ICU physicians were less likely to challenge a surgeon’s incorrect diagnosis when the surgeon was rude.1 More than 50 percent of respondents in a survey of more than 5,000 hospital staff “described the perceived negative impact of unacceptable behavior on teamwork as moderate or major; this effect was more prominent in nursing and allied health than medical staff.”1 Hicks and Stavropoulou reported that 13 to 45.5 percent of clinicians in the studies they reviewed “were aware of a specific adverse incident that had occurred because of DB.”2
Closing Thoughts
None of us can claim perfection in our interactions with colleagues and other HCPs, and all of us have behaved in ways that others could interpret as rude or impatient. While not intended to harm the other professional or reduce the quality of patient care, an awareness of the unintended effects of this behavior can motivate us to be more careful in all our interactions. Since it is human nature to be more circumspect in our interactions with higher-ranking individuals, we should take particular care in our interactions with more junior colleagues.
John T. Brinkmann, MA, CPO/L, FAAOP(D), is an associate professor at Northwestern University Prosthetics-Orthotics Center. He has over 30 years of experience in patient care and education.
To read more, refer to “Advocating or Disrupting?” in the December 2021 issue of The O&P EDGE that discussed disruptive behavior and made application to how O&P practitioners can function effectively as part of the healthcare team.3
References
- Guo, L., B. Ryan, and I. A. Leditschke, et al. 2022.Impact of unacceptable behaviour between healthcare workers on clinical performance and patient outcomes: A systematic review. BMJ Quality & Safety 31(9):679-87.
- Hicks, S., and C. Stavropoulou. The effect of health care professional disruptive behavior on patient care: A systematic review. Journal of Patient Safety 18(2):138-43.
- Brinkmann, J. 2021. Advocating or disrupting? The O&P EDGE 20(12):20-5.
Opener Art: jozefmicic/stock.adobe.com


{kind=link}