
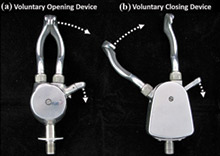
The VO device used in the study was the Sierra 2-Load hook (with custom extension added to make it the same length as the VC device); the VC device was the APRL VC hook, with clutch-lock disabled.
Photograph by study authors B. Kelsey, et al., courtesy of JRRD.
Persons with an upper-limb amputation who use a body-powered prosthesis typically control the prehensor through contralateral shoulder movement, which is transmitted through a Bowden cable. Increased cable tension either opens or closes the prehensor; when tension is released, some passive element, such as a spring, returns the prehensor to the default state (closed or open). A team of researchers aimed to determine whether using either a voluntary closing (VC) or a voluntary opening (VO) device makes a functional difference in activities of daily living (ADLs). Their longer-term goal was to assess whether providing the user with both VC and VO functions in one device would improve function. The study was published in volume 51-2 of the Journal of Rehabilitation Research & Development (JRRD).
According to the study, most body-powered split-hook prehensors used are VO devices, in which a passive spring closes the device and hence determines the grasp force. An advantage of VO prehensors is that, after actively opening the fingers and positioning them around an object, the user can relax because the spring provides the grip force to hold the object. However, the force generated by the VO prehensor is constrained by the spring strength. The user must thus select a spring strength based on the maximum grip force he or she anticipates needing; for example, a stronger spring is required for heavy, irregularly shaped, or slippery objects. This has two implications. First, the user must overcome a larger than necessary spring force and expend unnecessary energy to open the device when manipulating lightweight objects that only require a low pinch force. Second, the user cannot properly manipulate objects that require more grip force than the spring provides. Some VO prehensors allow the user to adjust spring tension but only over a limited range of forces.
VC devices use a spring to overcome friction and return the finger to the open state. With a VC device, users can control the grasp force and therefore only expend as much energy as is necessary to hold light, moderate, or heavy objects. However, the tradeoff for this increased grasp control is that the user must maintain the grip force while holding the object and generate force throughout the entire task, causing fatigue, unless the device has a clutch. However, a clutch must be disengaged at the end of each movement, requiring an additional control signal, and clutches often wear out before the prehensor.
The researchers used the Southampton Hand Assessment Procedure (SHAP) to examine functional differences between these two types of prehensors in 29 able-bodied subjects (who used a body-powered bypass prosthesis) and two individuals with unilateral transradial amputations (who used a conventional body-powered device). They also administered a survey to determine whether subjects preferred one prehensor or the other for specific tasks. The study used one VO and one VC device, which were chosen because they had identical fingers; using different fingers was found to noticeably influence results in a pilot study. In this study, task completion time, averaged across all of the tasks, and index of functionality (IOF) were the only objective performance measures assessed.
This study found that the VC prehensor performed slightly faster across tasks than the VO prehensor, but this did not result in a statistically significant improvement in the IOF. This study also provided insights based on a questionnaire regarding which features subjects preferred, depending on the task. Subjects had consistent preferences that made the VO prehensor better for some tasks and the VC prehensor better for others. Subjects agreed that a device that could switch between the two modes would be advantageous. The researchers concluded that “this information should…be useful both to clinicians for fitting and training patients and to engineers for designing new devices or optimizing existing ones.”


