

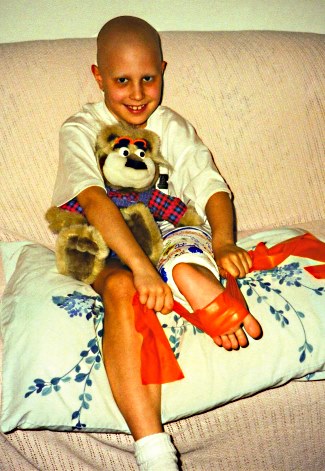
When she’s wearing pants, no one would guess that Shanna Decker has a prosthesis, much less that she had her left knee and part of her femur amputated many years before. At 25 years old, she can run, bike, ice skate, and participate in most sports as well as or better than any other practiced patient with a transtibial amputation, and she has a natural gait. However, the difference between her and other patients with amputations is apparent when she removes her prosthesis: Instead of seeing a knee, her foot is on backward with her ankle acting like a knee joint.
The procedure she underwent, called rotationplasty, saved Decker’s life from cancer and also gave her a future filled with sports and activities, which had once been unthinkable for someone with her illness and amputation.
“I’ve had it for 17 years and I’m just as mobile as I ever was,” Decker says. “It’s not impacting me or stopping me. It gave me my life.”
A Rare Procedure With an Unusual Appearance
Though rotationplasty has been around since at least the 1930s-when it was cited to treat a patient who had a severely shortened leg after tuberculosis of the knee-it became less obscure in the 1970s when it was first used with patients who had osteosarcoma. In 1974, physicians from the Orthopaedic University Clinic, Vienna, Austria, performed the first rotationplasty after a resection of osteosarcoma. During the operation, the section of the femur, knee, and tibia that are impacted by the cancer are removed. The remaining healthy lower part of the leg and foot are then rotated 180 degrees and fused to the femur, with the ankle functioning as a knee joint.
Though the result looks odd at first glance, it allows the patients to have a more natural gait and the foot to act as a weight bearing surface for which it was originally designed.
“It’s a function-sparing procedure,” says Mike Gozola, CP, who works for Hanger Clinic’s Rochester, Minnesota, patient care facility and has been working with this patient population since the 1980s. “It basically allows the patient to function as a below-knee amputee with all of the benefits that come with that, as opposed to putting a knee joint in.”
Patients who opt for transfemoral amputations generally don’t have the same kind of mobility, Gozola says. “So in terms of these kids, all of them are capable of returning to kid activities with virtually zero restrictions,” he says. “What they want to do, they do.”
Another benefit is that, generally, the patients do not experience phantom limb sensation or pain because they are still, for all intents and purposes, using their foot to walk. Though the procedure is becoming more common as surgeons have seen its successes, it will probably remain relatively rare because the cancer that prompts the surgery is rare, Gozola says.
Studies show that rotationplasty does work, he says. A 2014 retrospective study, published in the American Journal of Physical Medicine & Rehabilitation, that Gozola helped conduct with other professionals from the Mayo Clinic, Rochester, observed 12 patients over time who had the procedure. There were complications stemming from the cancer itself, such as chemotherapy delaying prosthetic fittings, but overall, the procedure, the patients, and their prosthetic outcomes were successful. “The findings of this study validate previous reports and confirm that most rotationplasty patients have excellent outcomes with return to premorbid physical activities,” the findings state.1
However, that’s not to say there aren’t drawbacks, Gozola says. The biggest drawback for most kids and their parents is the overall appearance after the procedure. “Kids at school can be mean,” he says. “The patients have to have a strong peer network because chances are they will be the only kids in their town with a foot on backward.”
What helps, he says, is that children with the procedure tend to be more mature than most children their age. “They have to mature a little bit faster than some of their peers,” he says. “They develop a little bit of a stoic personality because they’ve faced the angel of death and told him to go back.”
Decker’s Story
As a seven-year-old with osteosarcoma, Decker and her parents had to face a seemingly impossible decision: She could either live her life with a transfemoral amputation and face a lifetime of mobility issues, or get a rare procedure that involved her foot being placed backward where her knee had once been.
At the time, it sounded ridiculous, she says. “I think my initial reaction was that this is absolutely nuts,” she says. “I was thinking, ‘They don’t really do that, do they?'”
All they had to help make the decision were black and white pamphlets that were published in Vienna and included pictures taken during the surgery. Still, the prospect of having better mobility was too important for an athletic child to pass up, she says, and they opted for rotationplasty.
After the surgery, she was surprised by her new look, but doesn’t think her reaction was much different than other patients who have under gone amputations. “I think my reaction to it wasn’t a lot different than if I had a regular amputation. The grief came from having something happen to my leg, in general, more than the look of the specific area,” she says. “But I got over it. That’s the benefit for young people; it’s easier for them to accept.”
After she finished chemotherapy and was fitted with a prosthesis, she learned how to walk again with her new “knee” and was soon off and running. “I do sports, I hunt, I hike-I do everything I would have been able to do otherwise,” Decker says. “It’s pretty incredible to be able to do that.”
Her athleticism helped her build muscle in her impacted limb and now her ankle is so muscular, it’s almost the size of her other knee, she says, and functions just as well. With the help of a physical therapist, she learned about how her body was compensating with the prosthesis, and she was able to improve her gait even more.
“When I’m wearing pants, people literally have no idea I have a prosthetic until I tell them,” she says. “I think a lot of that credit goes to the gait.”
She has dedicated herself to spread the word about the procedure and give help and support to families dealing with childhood cancer. Physicians turn to her to talk to potential candidates and let them know what they can expect. “I haven’t seen more than one [procedure] ever fail, and that didn’t have anything to do with the prosthesis; it was that the surgery was done incorrectly,” she says. “Otherwise every person will tell you that it’s the best decision in their life. I was able to do everything I wanted to do.
The Importance of a Good Fit
Stephen Miller, CPO, regional vice president of Hanger Clinic, Savannah, Georgia, knows firsthand how important a good prosthetic fit is for patients who have undergone rotationplasty.
As a boy, he was knee-boarding behind a boat when he realized that he couldn’t bend his knee all the way. His parents took him to a physician and he was diagnosed with osteosarcoma.

“They said, ‘We don’t want to take a chance, we have to take the leg above the knee. We can do some limb salvage or we can do this procedure called rotationplasty,'” Miller recalls. The family opted for rotationplasty without knowing much or even seeing a picture of what it would look like. Miller was fitted for his first prosthesis and, as an active child who didn’t want to slow down, he soon found himself in trouble with a bad prosthetic fit. “The first prosthesis I had was atrocious,” he says. “If I ever tried to play a sport or run, there were blisters. It was terrible; it would put my parents in tears.”
His parents soon found a prosthetist who had experience with the procedure and the result was immediate, Miller says. “I tell you, he made me a prosthesis and from that day on I knew the importance of a good-fitting prosthesis and how it can change your life,” he says. “I played every sport, hiked, water skied, and snow skied. The only difference between me and my peers was that I couldn’t run as fast.”
The difference in his life was so profound, he says, that it inspired him to become a prosthetist and help other children with the procedure. Since rotationplasty is rare, and still relatively new, there aren’t a lot of prosthetists with experience fitting these patients. Some who attempt it, he says, don’t always do their due diligence before they attempt to fit a patient.
“I’ve seen some terribly designed prostheses and those parents think that they made a mistake [with the surgery],” Miller says. “[The parents] chose a prosthetist who was recommended to them, and because they are good prosthetists they think they can do the rotationplasty, but they don’t really know what they are doing.”
Left untreated, a bad fit can lead to pain and other complications. One of the most common, he says, is verrucous hyperplasia-thick, raised, and itchy tissue over the patient’s toes. This is usually because the prosthetist does not know how to protect and fit the toes within the prosthesis.
Many times, problems last longer than they should because children, who make up the majority of rotationplasty patients, are less likely to complain and more likely to push through the pain than adults would, he says.
“Some kids can walk on anything,” Miller says. “They just want to keep on playing. It’s our responsibility to keep an eye on them and work for their long-term success.”
The key, says Miller and Gozola, is the same as for other prosthetic devices: a good socket fit. “As in any prosthetic device, if the socket fits, you can have a broomstick and do well,” Gozola says. “Or you can have expensive componentry and if a socket doesn’t fit, you just have an expensive flower pot.”
Understanding the anatomy of the ankle, and its differences compared to the knee, is the most important part of fitting these patients well, they say. “It’s an ankle, it’s not a knee,” Miller says. “The anatomy is much different. You have to protect the integrity of the ankle joint, the integrity of the skin, the integrity of the toes, and you have to realize the limitations with an ankle. It doesn’t bend past 90 degrees.”
Also, Gozola points out, anyone who watches a woman wobble in high heels can see that the ankle is not a stable joint. “You can’t just put a socket on the foot because of the inherent instability of the ankle,” he says. “You have to support the ankle joint with below-knee joints up to the thigh.”

As he has seen rotationplasty patients over the course of several years, or even decades, Gozola says he has also learned to take much more initial care in fitting around the foot. “The top of your foot is usually something you put your shoe over,” he says. “With these patients, their foot is going up and down and the tendons are exposed. As the foot becomes older it becomes a point for potential problems. Now we spend a lot more time fitting the dorsal aspect of the foot, making sure there is relief for any bony prominence. We are bending the foot over sideways, making things stick out, and trying to have room for all of the things that happen to the top of the foot. You have to be careful that they don’t get pressure where there shouldn’t be any.”
Learning to fit these patients can be tough, Gozola says. “They don’t teach it at school because they can’t. Most [prosthetists] will see maybe one patient in their entire career…. There’s no place to learn it. Right now, it’s like the old Eskimo traditions where they had to pass their knowledge on to youngsters.”
Both Miller and Gozola say interested prosthetists should always contact others if they have questions. “If I had my first rotationplasty patient, I would reach out to other prosthetists around the country that have experience and gain as much information as possible,” Miller says. “I’m happy to send over my PowerPoint presentations, do FaceTime, or whatever I can do to help.” If a practitioner is still unsure, he or she should probably refer that patient to the place where they can get the best care, he says.
Looking Toward the Future
With the rarity of the procedure, there aren’t a lot of adult patients to test the long-term impact of rotationplasty. For the few who have decades of experience, things seem to be going well. Gozola says his oldest patient is 41 years old and she still feels, after all this time, that she made the right decision. “She would never consider having her foot cut off-never,” he says. “None of the kids have opted to have a surgical revision.”
Miller says he too is still doing well decades after his rotationplasty surgery. “I’m 41 years old; I have zero health issues,” he says. “My foot is in perfect condition.”
Decker is also still doing well physically, though she now wears an orthotic on her rotated foot to help the arch, which has been falling as she has aged. Physical therapy and staying active and healthy have also helped her avoid complications, she says. Personally, she has adjusted well and feels that rotationplasty was the best thing she could have done. She mentors children with cancer and gives advice to anyone who asks about the procedure.
“I’m in a relationship with a physical therapist and he thinks my leg is fantastic,” she says.
As time goes on and bodies change as they age, there are still a lot of unknowns, Decker says. “The honest truth is that they don’t know. We are the long-term study. As we grow and adapt, the prosthetist also has to grow and adapt.”
Maria St. Louis-Sanchez can be reached at msantray@yahoo.com.
Reference
- So, N. F., K. L. Andrews, K. Anderson, M. A. Gozola, T. C. Shives, P. S. Rose, W. J. Shaughnessy, and F. H. Sim. 2014. Prosthetic fitting after rotationplasty of the knee. American Journal of Physical Medicine & Rehabilitation 93:4: 328-34.


