
Communication between healthcare providers and patients or caretakers is the foundation of effective clinical care. Information exchanged during initial evaluations and follow-up appointments forms the basis for accurate identification of problems and specific treatment recommendations. This is especially true for orthotists and prosthetists, who rely primarily on patient reports and clinician observation rather than standardized assessment or diagnostic tools. Every orthosis and prosthesis must be worn to be effective, and proper wear and use often determine outcomes. Reduced wear time of some devices may be appropriate, and patients who properly wear their upper-limb prosthesis or lower-limb orthosis for less time that we recommend could be considered adherent. In other cases, such as positional cranial deformities and scoliosis, proper wear of an orthosis for a specific time (dosage) is essential to achieving treatment outcomes, and reduced wear time constitutes nonadherence. Accurate wear time reports are necessary in these populations to determine whether changes to fit, design, or outcome expectations are appropriate.
Determining the cause of device fit, function, and durability problems also requires truthful and transparent accounts of specific behaviors and habits from patients and caretakers. For a variety of reasons, patients may not recall or may choose to withhold important information related to these behaviors, particularly if it does not reflect well on them. When the veracity of a patient’s account is in question or demonstrably false, practitioners are not only inhibited in their ability to provide effective care, but may also distrust and resent the patient. This can depend on whether the patient’s memory or their character is assumed to be the source of the inaccuracy. Not all misreporting is intentional or done with the intent to deceive, and our assessment of the likely root of the misinformation can affect our ongoing clinical interactions with that patient.
Several examples from my experience can help to identify the nuances of interpreting incomplete or inaccurate information from patients. I find it easy to assume that elderly patients’ misreports are caused by age-related memory loss or more serious dementia, rather than an attempt to deceive. Exaggeration of wear times in scoliosis, cranial remolding, or pectus carinatum cases are more understandable (and forgivable) given the extended wear times required during a challenging stage of life. Inaccurate reports of wear and care behaviors often appear to be related to a lack of familiarity with a new or different device. For example, in some cases of persistent skin irritation, patients have insisted that they were cleaning the prosthetic liner in the recommended manner. In each case, I asked the patient to note when and how he or she cleaned the liner each day and return in one week. When the skin irritation had resolved by the time of the follow-up appointment, the patient acknowledged (somewhat sheepishly) that previous cleaning of the liner had not been done as much as he or she thought. The willingness to accept responsibility seemed to indicate a genuine inability to recall the specifics of their daily habits.
Other examples appear to be related to intentional misrepresentation. Two suspicious reports related to damage to a prosthesis remain clear in my mind many years after they occurred. In one case the crushing damage to a transtibial socket was inconsistent with the patient’s claim that the damage occurred when he jumped off a rock while hiking. (Such severe damage to the socket while it was worn would have resulted in significant physical injury.) In the other case, the patient had been paid directly by his insurance company for replacement of a damaged prosthesis at some point in the past, and his reports of damage to his current prosthesis were vague and inconsistent. After persistent questioning, he eventually admitted that he needed money and asked me to document that his current prosthesis was damaged so that he could receive another payment from the insurance company. His offer to split the proceeds of this fraudulent endeavor with me did not increase my trust in him or result in a continuation of the clinical relationship. In these two cases, I interpret the misrepresentation as lying for the purpose of financial benefit. In the earlier examples, it is easy to see other factors, including memory lapses and embarrassment about nonadherence, as contributing to the inaccurate reports. It seems important to view those misreports differently.
Memory in Everyday Life
Research on memory of daily events provides interesting insights into our patients’ accounts of their behaviors and habits. Although not every event is remembered, there is a high degree of accuracy of remembered events days or months after they occurred.1 Episodic memory is “the ability to store and recall events within a specific temporal and spatial context, enabling individuals to remember personal experiences and their details.”2 Prototypical memory is not tied to a specific event but a standard or representative example of an event. Diamond et al. used the example of a morning commute, the details of which, on any particular day, may only be remembered if they deviate from the normal experience.1
It is likely that patients may not recall a daily wear and care routine with as much accuracy as when that routine is disrupted by unusual events (such as a specific fit or function problem). They may recall a general time frame when a specific problem first occurred but not recall as accurately the behaviors (for example, sock management, donning/doffing schedule, cleaning practices) that they consider normal but may have contributed to the problem. Recognizing this helps us to distinguish between an intent to deceive practitioners about their behaviors and difficulty remembering behaviors that are part of their usual routine. When we ask for more detail about specific events and behaviors (episodic memory), patients may report their usual practices and routines (prototypical memory).
Lying
Patient reports that are inconsistent or do not match the evidence we observe may be intentional misrepresentations. Intentional misreporting can involve leaving out relevant information or stating falsehoods. According to a 2019 news article by Lauren Vogel in the Canadian Medical Association Journal, “In two recent national surveys of 4,510 Americans, 60-80 percent admitted they had not been forthcoming with doctors about information that could be relevant to their health.”3 Additionally, “85 percent of patients admitted to concealing or fudging the truth, and roughly a third lied to their doctors. A recent survey of Americans insured under Medicare Advantage plans found that 47 percent lied to their doctors, mostly about their diets, exercise habits, sex lives, or adherence to treatments.”3 Reasons given for this include disagreement with a doctor’s advice, not understanding treatment instructions, and when “asked why they didn’t tell the truth, most said they didn’t want the doctor to judge or lecture them. More than half said they felt embarrassed. Respondents also said they didn’t want to be ‘difficult’ or to waste the doctor’s time.”3
In my experience, most instances of patient misreporting are not motivated by financial gain. However, it is common for patients to express dissatisfaction with a device (and perhaps even the skills of a practitioner) when their own unreported nonadherent behavior has contributed to the problems they are experiencing.
Patient Reports of Nonadherence
Given the many factors that contribute to the accuracy and forthrightness of patient reports, it is perhaps even more interesting to consider why and how patients report “acting in a way that is out of line with medical advice.”4 In their 2013 paper, sociologists Clara Bergen, PhD, and Tanya Stivers, PhD, borrowed the following definition of a patient disclosure: “the act of seeking care by revealing personally significant information that exposes the bearer to the risk of rejection or negative judgment.”4 They reported that in about half of disclosures, “the patient has been interactionally ‘cornered’ by a physician’s question since answering the question requires the patient to either disclose nonadherence or lie, to a greater or lesser extent….”4 It is important to remember that as incomplete as the disclosed information may be and as frustrated as we are with reports of nonadherence, patients are making a difficult moral choice to share self-incriminating information that can help us provide more effective treatment.
Bergen and Stivers focused “on cases where patients report wrongdoings in ways that show them to be aware that their behavior is at least potentially problematic from a medical perspective.”4 They analyzed “268 video-recorded primary care visits,” of which 57 included “at least one patient-acknowledged misdeed….”4 They found that “when disclosing misdeeds, patients characterize their behavior using negatively valenced words…[and] commonly exhibit speech dysfluencies when reporting behavior as problematic (hesitant speech, stretching sounds, stuttering, pauses, reformulations)….”4 This is consistent with research showing that “dispreferred actions” in conversations (e.g., disagreement or not answering a request for information) “tend to be delayed, commonly have production hitches and perturbations, frequently include hedging and mitigation,” all of which “convey an iconic reluctance to move forward.”4 The researchers pointed out that “these features are also frequent in disclosures, suggesting here too a reluctance to progress through the turn—evidence that speakers are oriented to the reported behavior as problematic.”4
By attending closely to patients’ word choices and their hesitancy to reveal their thoughts or feelings, practitioners may be able to detect that patients are orienting “their behavior reports not as neutral reports but as disclosures of problematic behavior.”4 When this occurs, responding in ways that increase the patient’s comfort and trust is more likely to result in more meaningful detail from the patient than stern repetitions of instructions.
In Bergen and Stivers’ study, 53 percent of the disclosures “were in response to a physician’s direct question regarding some potentially problematic behavior,” and 47 percent were initiated by the patient.4 They pointed out that in initiating disclosure “patients display agency insofar as they are providing a report of new information that has not been explicitly requested by the physician…and in having performed some medically relevant action against or without medical advice.”4 While we correctly identify the health behavior as a misdeed, we can respect and encourage the patient’s agency. After all, they could have chosen not to reveal the misdeeds, which would leave us with less information on which to base future recommendations and treatment. Further, any meaningful change in their behavior will require their agency. Affirming and guiding their agency is likely to improve outcomes more effectively than directly confronting its misguided application.
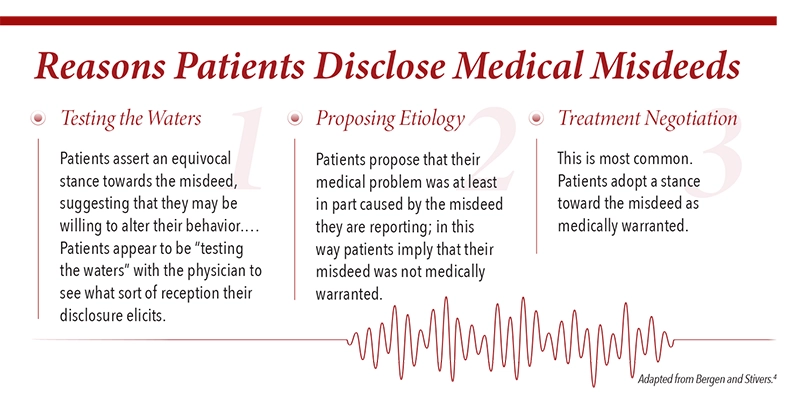
Bergen and Stivers reported that patients in their study asserted their agency by disclosing medical misdeeds. “Through this practice, patients convey that they are willing to make unsanctioned lifestyle choices, alter their treatment regimens without seeking their physicians’ advice, disregard physician recommendations, propose causal explanations for health outcomes, and lobby for alternate treatment recommendations.”4 Again, the fact that their choices were not optimal, and may even have gone directly against our recommendation, may be less important than the fact that they shared the information with us.
When patients make the difficult choice to reveal information rather than conceal it, this may reflect ambivalence about their care. They may be seeking clarification on our opinion and recommendations so that they can make informed decisions. They may be aware that their misdeed has contributed to a health problem and recognize an obligation to follow our recommendations and adhere to the treatment plan. “Patients show themselves to be oriented to their lack of cooperation as inappropriate but do it nonetheless. Thus, contemporary patients exhibit an ambivalence about the role they want to and should play in their own healthcare, somewhere between passive patient and proactive consumer yet not quite a shared decision-making equal either.”4
Closing Thoughts
If we view ourselves as responsible only or primarily for the provision of an appropriately fitting and functioning device, we may not see the opportunities that arise through patient disclosures of their misdeeds. If, on the other hand, we acknowledge a more holistic responsibility toward our patients, including coaching and supporting their behavior change, we will begin to view disclosures as an opportunity to navigate ambivalence with patients and guide them toward healthier behavior.
Learning to recognize the signs of disclosure can help us adjust our response to encourage more transparency from patients. John Palmieri, MD, and Theodore Stern, MD, advised that practitioners should “focus on the creation of an environment that fosters honesty…. It is unrealistic to expect all patients to risk punishment, rejection, and humiliation without first setting a tone of tolerance, workability, and the capacity to accept ambivalence.”5
John T. Brinkmann, MA, CPO/L, FAAOP(D), is an associate professor at Northwestern University Prosthetics-Orthotics Center. He has over 30 years of experience in patient care and education.
References
- Diamond, N. B., M. J. Armson, and B. Levine. 2020. The truth is out there: Accuracy in recall of verifiable real-world events. Psychological Science 31(12):1544-56.
- https://www.sciencedirect.com/topics/psychology/episodic-memory
- Vogel, L. 2019. Why do patients often lie to their doctors? CMAJ 191(4):E115.
- Bergen, C., and T. Stivers. 2013. Patient disclosure of medical misdeeds. Journal of Health and Social Behavior 54(2):221-40.
- Palmieri, J. J., and T. A. Stern. 2009. Lies in the doctor-patient relationship. Primary Care Companion to the Journal of Clinical Psychiatry 11(4):163.




{kind=link}