
Introduction
Approximately 133,000 amputation-related hospital discharges occur each year in the United States, 31 percent of which are at the transfemoral level.1 The healthcare team’s primary concerns for new amputees are assessing and improving their mobility. In a study of 25 lower-limb amputees, Deans et al. found that there was a significant relationship between amputees’ functional ability and their physical, psychological, and social well-being.2 This finding shows that an assessment of the patient’s functional development throughout the recovery process is instrumental to his or her community reintegration. However, there has been very little research regarding prosthesis use after discharge and if the function attained through prosthetic intervention is maintained thereafter.
Technological advances in prosthetic devices such as energy-storing feet, microprocessor-controlled knees, ankle rotators, and shock absorbers have attempted to mitigate negative functional effects associated with prosthesis use. However, van der Linde et al.’s literature review highlights a lack of unbiased information about the direct effects these components have on a patient’s functional ability. Only two significant comparative studies were found on the effect that prosthetic feet and knees have on gait.3 The vast majority of clinical studies have used standardized gait-assessment protocols with limited ecological validity, making them inappropriate to use when prescribing a prosthesis.3 More research is needed to illustrate the long-term functional impact of prosthetic training on persons with lower-limb amputations and the use of advanced prosthetic components.
Each phase of amputee rehabilitation has distinct challenges, goals, and outcomes (table 1). The purpose of this case report is to show the functional development of one patient from prosthetic training stage to follow-up, with quantitative and qualitative assessments of functional status at various intervals.
Case Presentation
The subject of this case report is a patient at Dayton Artificial Limb Clinic, Beavercreek, Ohio. The patient is a 54-year-old female with a right mid-transfemoral amputation, is 5 feet 9 inches tall, and weighs 188 pounds. Her August 2008 amputation was the result of a Methicillin-resistant Staphylococcus aureus (MRSA) infection contracted during her fifth knee-replacement surgery. Also of note, the patient fractured her pelvis and sacrum in a 2008 fall, has occasional seizures as a result of a 1989 head trauma, and recently had a cyst removed from her contralateral meniscus. Shortly after the amputation, she was fit with a prosthetic leg through another prosthetics company. The patient did not receive any physical or occupational therapy following this fitting; she was instructed on how to use the prosthesis and released. The patient experienced a great deal of pelvic pain and therefore wore her prosthesis infrequently, opting instead to use a walker and a wheelchair to navigate her one-story home, where she lives alone. She attends church service once a week, does her own grocery shopping, and is able to perform light household maintenance tasks independently. She is currently unemployed. She smokes a half of a pack of cigarettes daily and drinks no alcohol.
In the prosthetic prescription stage, the referring physiatrist classified the patient’s ambulatory status as a K3, indicating her potential to achieve ambulation with variable cadence, negotiate most environmental barriers, and use a prosthesis beyond simple locomotion.4 The physiatrist discussed his recommendation with the patient, who reported an active lifestyle prior to her amputation. Considering that Taylor et al. found that functional status prior to the development of limb symptoms is the best predictor of post-rehabilitation performance, a long-term prosthetic prescription including high-activity components was created.5 The prescription called for an initial fitting with a manual locking knee and eventual progression to a microprocessor knee.
The patient began prosthetic training in July 2010 and presented with a hip flexion contracture, which was immediately and aggressively addressed since its presence has been shown to be one of the most significant predictors of a poor prosthetic outcome.6 Due to her mid-transfemoral amputation and history of hip fracture, the primary concern during prosthetic training with this patient was dynamic stability and fall prevention. Although usually recommended for geriatric patients, the patient was fit with a manual locking knee during the first stage of prosthetic training because it maximizes dynamic stability. The prosthetist mounted a 15-degree Flexcon offset plate to the distal end of the socket, which reoriented her trochanter-knee-ankle line to fall anterior to prosthetic knee center, thereby maximizing stability. Since a manual locking knee was being used, the additional 15 degrees of socket flexion that the Flexcon provides was a key feature of this component choice. The Flexcon also provides anterior offset of the socket in relationship to the knee component. The magnitude of the anterior offset is calculated based on the degree of flexion in the plate (15 degrees) and the approximate length of the patient’s residual limb (8 in., 10 in., 12 in.).
The prosthetist decided that the best course of action was to fit a vacuum chamber socket design (VCSD), which is conducive for use with either passive or active vacuum fittings. For this particular case, a passive vacuum socket fitting was found to be the best option for the patient. Passive vacuum was obtained via use of the Elevated Vacuum Locking System™ (EVLS™), SealMate™ silicone locking liner, and Aura Locking Sheath along with the EV-MAN-VLV, which is a combination air-transfer manifold and slide-operated release valve.


Upon evaluation of the patient for a silicone locking liner, the prosthetist determined that the circumferences at 5cm (2 in.) proximal to the distal end and at the perineum were 55cm and 71.5cm, respectively. Because of the difference between these two measurements, the prosthetist decided that an off-the-shelf liner would not be adequate. The patient was cast and measured for a custom SealMate silicone locking liner to properly accommodate the soft tissue of her residual limb.
Once the patient was fit with the custom liner, a passive casting technique was employed to capture the pelvic anatomy and residual limb soft tissue. The cast was taken by applying casting pants or equal barrier to cover the patient’s skin and liner. The landmarks identified for this casting procedure were the apex of the greater trochanter, ischial tuberosity (IT), and adductor longus tendon. A coronal limb bisector was used to align the European four-hole bolt pattern. Any other trigger points and/or bony areas were also noted. Although the patient was cast while she was standing, she also could have been cast lying on her non-involved side with her residuum abducted with limb and soft tissue support.
To start the casting procedure, we made a 5-7 layer splint of rigid 6-in. plaster bandage. The splint was long enough to cover the adductor longus to the IT from anterior to posterior. Once the splint was applied, it was only necessary to capture the natural anatomy of the perineum; definition of the IT is not desired in this casting method. The final socket posterior trim line should be more gluteal weight bearing than IT/ramus containment. The shape capture of the inferior-medial aspect of the gluteus maximus is more important. Once the splint was in place, the limb was circumferentially wrapped with a 4-in. flexible plaster bandage followed by the same with a 4-in. fast-setting rigid plaster bandage. The limb was wrapped in abduction to allow for easier access; once the rigid bandage was in place, the limb was returned to the neutral position. Once set, the cast was removed and prepped for imaging for import into the CAD program.
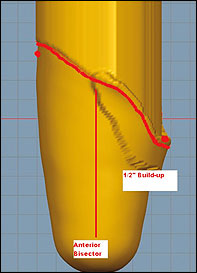
We used a Provel (Seattle, Washington) D1 mechanical point digitizer to obtain a digital image/model of the cast impression. The socket model was then imported into an industry specific CAD program for modifying. Following a blending procedure to remove any abnormalities, landmarks were added every 2 in. below IT level. The circumferences of the model were then scaled down to 96 percent for a 4-percent circumferential reduction. Following reduction, the trim line was added to the model. (See figures 1 and 2.) The trim line is used to help us plan where to apply our build-ups, which mostly serve to supply relief for hip flexor and adductor contractions during the gait cycle.
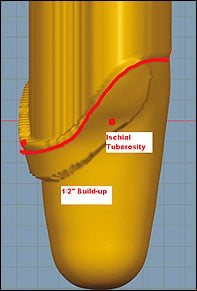
The initial build-up was adding 1/2-5/8 in. of relief from the midpoint of the proximal anterior at the trim line medially to the adductor region (figure 3). This build-up runs medial to posterior around the region where the IT was marked (figure 4). The build-up is applied at the trim line and 1-1.5 in. below it and is then blended/tapered distally to allow for a smooth transition. More or less build-up can be applied based on patient muscle tone and tissue density in these regions.
The reduction of circumferential measurements and the proximal build-up are the only modifications required because of the superior linkage and rotation control that the combination of the Aura Locking Sheath and vaccum provide.
We then added the necessary tooling so that there would be a void in the socket for the EVLS, which acts as a suspension aid, distal socket seal, and connecting plate. Formation of the distal void is of the utmost importance to ensure a quality seat at all sealing points between the socket and EVLS lock.
We tested the seal quality of the finished definitive socket by installing the EVLS lock and manifold, applying a vacuum source (up to 27 in Hg), and ensuring the distal end of the socket is sealed. The proximal aspect of the socket will be sealed through use of the Aura Locking Sheath and coverless SealMate locking liner.

Within 15 minutes of training with the new prosthesis, the patient was able to push off with the prosthetic foot, and she had better than expected swing phase symmetry—even with the locked prosthetic knee. She walked with her left hip retracted and her sound side adducted, in part due to two years of walker use. These initial gait abnormalities are common manifestations of a hip-flexion contracture, including knee instability, lordosis, and uneven step length.
To improve the patient’s gait, we first had her walk more slowly and spend more time in double support. This action reflects research done by Kendell et al., who recognized those two adjustments as the most effective ways to increase dynamic stability with a lower-limb prosthetic device.7
We chose the Locomotor Capabilities Index (LCI) as the functional outcome measure in this report. Consisting of 14 basic and advanced activities and a five-point ordinal scale, the LCI is designed to measure a lower-limb amputee’s capabilities with a prosthesis during and after rehabilitation. The LCI has demonstrated good internal consistency, test-retest reliability, construct validity, and is widely used for clinical and research use with amputees.8,9
After the patient’s first prosthetic training appointment, we conducted an interview with her, which included the administration of the LCI and Independent Activities of Daily Living Scale (IADL) assessments. The IADL evaluates the amputee’s ability to perform eight different daily activities. The patient is rated with a score of 1 or 0 on each activity.10 She scored a 17 out of a possible 56 points on the LCI, earning 11 points on the general tasks and six points on the advanced tasks. She scored six out of a possible eight points on the IADL.
On her second prosthetic training visit, we replaced the Flexcon with an offset plate. This decision was made with the recommendation of the physical therapist, who said that the flexion contracture had been sufficiently reduced. After four prosthetic training sessions, the patient scored a 12 on the LCI, indicating that her judgment of her abilities with the prosthetic leg had become more realistic with training. This is consistent with Gauthier-Gagnon et al.’s note that the LCI does not measure the amputee’s actual performance, but rather his or her perceived capacity.8 At this same appointment, the patient scored a seven out of eight points on the IADL. This assessment measures the amputee’s actual performance rather than his or her perceived capacity. After two months with the prosthesis, the patient scored a 19 on the LCI, with 17 points on the general tasks and two points on the advanced tasks. This is an improvement of seven points from her more realistic score of 12 after her first four sessions of prosthetic training.
Discussion
This patient achieved mobility much sooner than other patients who display the same type of hip flexion contracture. The following widely used physical therapy interventions for hip flexion contracture were used with this patient: backlying with neutral hip extension, lying prone with a 6-in. diameter rolled towel placed under the patient at mid-femur, and stretching in the form of forward pelvis rotation while in approximate midstance. After low-load continuous stretching, more aggressive contract-relax exercises were employed to lengthen the hip flexor. These exercises reduced the angle of the hip by 5 degrees after the first session. Use of sagittal isometric contract-relax treatment of a contracted muscle with an amputee was not found in the literature review. Traditionally, the flexion contracture can only be addressed therapeutically, but the recent development of the Flexcon offset plate allows the prosthetist to immediately reduce the negative effects of flexion contracture on gait so the patient can begin gait training with the prosthesis much sooner. Therapeutic interventions continue, and, as seen with this patient, the Flexcon plate is removed when the patient has improved range of motion at the hip.
Tracy Slemker, CPO, is the founder of Prosthetic Design Inc. (PDI), Clayton, Ohio. In business since 1991, PDI focuses on CAD-CAM integration through modular parts and production materials.
Author’s note: Written, informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by contacting the editor in chief of this publication.
References
- Gailey R, Allen K, Castles J, Kucharik J, Roeder M. Review of secondary physical conditions associated with lower-limb amputation and long-term prosthesis use. J Rehabil Res Dev. 2008; 45(1): 15-30.
- Deans SA, McFadyen AK, Rowe PJ. Physical activity and quality of life: A study of a lower-limb amputee population. Prosthet Orthot Int. 2008;32(2):186-200.
- van der Linde H, Hofstad C, Geurts A, Postema K, Geertzen J, Limbeek J. A systematic literature review of the effect of different prosthetic components on human functioning with a lower-limb prosthesis. J Rehabil Res Dev. 2004;41(4):555-570.
- Ip D. Orthopedic Rehabilitation, Assessment, and Enablement. Heidelberg, Germany: Springer-Verlag; 2007.
- Taylor S, Kalbaugh C, Cass A, et al. “Successful outcome” after below-knee amputation: An objective definition and influence of clinical variables. Am Surg. 2008;74:607-613.
- Munin M, Guzman M, Boninger M, Fitzgerald S, Penrod L, Singh J. Predictive factors for successful early prosthetic ambulation among lower-limb amputees. J Rehabil Res Dev. 2001;38(4):379-384.
- Kendell C, Lemaire ED, Dudek NL, Kofman J. Indicators of dynamic stability in transtibial prosthesis users. Gait Posture. 2010; 31(3):375-379.
- Gauthier-Gagnon C, Grisé M. Tools to measure outcome of people with a lower limb amputation: Update on the PPA and LCI. J Prosthet Orthot. 2006; 18:1.
- Condie E, Scott H, Treweek S. Lower Limb Prosthetic Outcome Measures: A Review of the Literature 1995 to 2005. J Prosthet Orthot. 2006;18:13.
- Lawton MP, Brody EM. Assessment of older people: Self-maintaining and instrumental activities of daily living.” Gerontologist. 1969;9:179-186.
- Esquenazi A. Amputation rehabilitation and prosthetic restoration. From surgery to community reintegration. Disabil Rehabil. 2004;26(14/15):831-836.



