
A student approached me after a behavioral science lecture a few years ago with concerns about something she had observed while shadowing at a facility prior to beginning her O&P education. She described being shocked by overhearing practitioners talk disrespectfully about patients. It was obvious that this caused her considerable distress, even many months after it happened. She asked, “Why would they talk that way about their patients?” I immediately thought of times I’d been part of similar conversations and I wondered if the issue was that this student’s idealism was, for the first time, bumping up against common frustrations involved in providing care. There is often a gap between appropriate professional attitudes and behaviors and our ability to maintain those standards, particularly in challenging clinical situations. I expect that it is common for practitioners to express negativity out of the patient’s earshot. How often do those discussions cross a line of professionalism, and how do they influence less experienced clinicians?
A questionnaire published by the Association of Medical Colleges reported that “one in five medical school graduates in 2016 reported experiencing ‘disconnects between what I am taught about professional behaviors/attitudes and what I see being demonstrated by faculty’ as frequently as fairly often (9.6 percent), very often (7.8 percent), or always (3.6 percent).”1 According to another source, “98 percent of [medical] students heard physicians refer to patients in a derogatory manner, 61 percent witnessed what they believed to be unethical behavior by other medical team members, 67 percent felt bad or guilty about something they had done…, and 62 percent believed that some of their ethical principles had been eroded or lost” during the clinical portion of their education.2
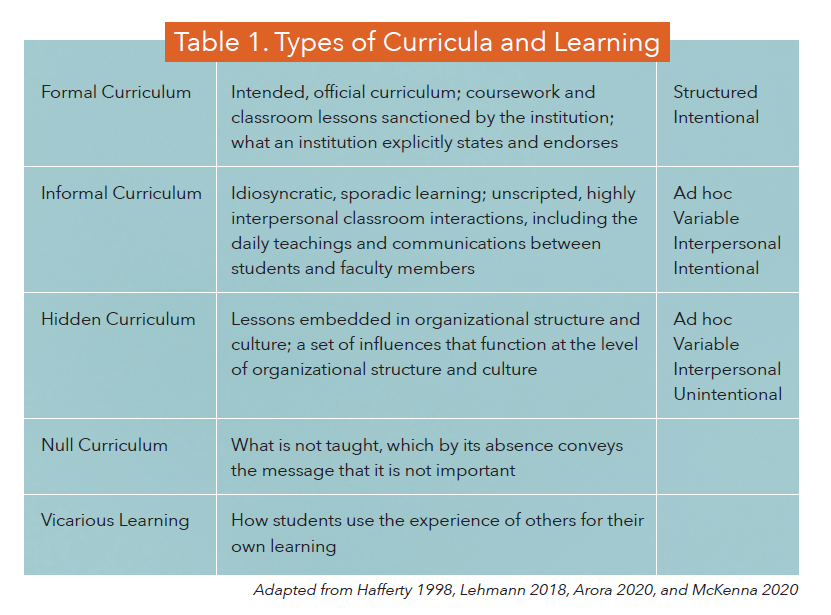
Education in any context involves a formal curriculum that includes content approved by the institution. What is taught in informal or hidden ways may or may not be consistent with this formal presentation of content and values (Table 1). For instance, common negative attitudes and behaviors that are not taught (and may not even be acknowledged) in a formal curriculum may be part of a hidden curriculum that has a significant impact on trainees. This hidden curriculum “exists beyond the classroom and is sensed in hallway conversations and subtle behavioral interactions, but never explicitly documented.”3 This article discusses the impact of the hidden curriculum on students and residents.
Definition
In addition to the formal and informal curricula, students also learn vicariously by observing and interacting with others. These methods are intentional and explicit and are common ways of communicating information and values. The term “hidden curriculum” was first used in 1968, but this phenomenon was described much earlier by educators.4 According to nurse and researcher Lisa McKenna, PhD, teaching and learning in the hidden curriculum involves a lack of intentionality and awareness: “Some of what students learn may not necessarily be what educators intend, and educators may be unaware of the full scope of what they are teaching students, namely, through their behaviors and actions.”5 Hidden instruction can be more powerful than that which is explicit and intentional.
Professional Identity Formation
One reason that the hidden curriculum deserves serious consideration is that medical education involves more than the transmission of knowledge and skills; “it is also a socialization process” whereby trainees learn what it means to be a professional in a particular discipline.2 According to McKenna, “studies have suggested that students value the informal, hidden curriculum in developing their professional roles.”5 For example, third- and fourth-year medical students in Australia were interviewed “about their perceptions of the hidden curriculum” and reported that “it was through this learning that they actually learnt about how to behave as doctors.”5 Another study reported that “students described how they learnt about power and hierarchy in the hospital and their role within that” through the hidden curriculum.5 In developing their sense of professional identity “trainees learn much more from modelled behaviors than from the formal teachings they receive.”3 The hidden training “is considered ‘sticky knowledge,’ more memorable than the explicit formal curriculum. Every word spoken, every action performed or omitted, every joke, every silence, and every irritation imparts values we might never have intended to impart.”2
The hidden curriculum may be one reason that negative attitudes increase as students progress through the medical
education process: “Students move from being open-minded to being closed-minded; from being intellectually curious to narrowly focusing on facts; from empathy to emotional detachment; from idealism to cynicism; and often from civility and caring to arrogance and irritability. This erosion of empathy and ‘vanquishing of virtue’ is repeatedly documented in studies of physicians in training.”2 No doubt some of the responsibility for these changes rests with the trainees themselves and may be an unfortunate (and not completely avoidable) consequence of increasing interaction with the difficult aspects of real-life clinical practice. However, we should also consider how the behavior modelled by experienced clinicians contributes to these negative transformations.
Ethical Dilemmas
The expectations of professional practice are described in accreditation and credentialing documents, and often take the form of official company policies. However, practitioners frequently must navigate situations that cannot be addressed by a formal policy. Many compromises practitioners must make between competing ethical obligations do not necessarily constitute ethical violations. These situations are called dilemmas precisely because there is not a clear, simple solution. By providing explanations about the relevant factors influencing their decisions, experienced practitioners can help trainees understand the nuances of ethical dilemmas in a way that prepares them to make difficult decisions in the future. Failing to provide explanations of the decision-making process may unintentionally teach trainees to disregard policies they do not understand or view as unimportant. The informal curriculum can be used to make decisions explicitly, while keeping them appropriately behind the scenes rather than completely hidden and unacknowledged.
How It Looks in Practice
There are many situations in which no reasonable rationale exists for behaviors and attitudes that clearly fall outside the standards of professional practice and official policy. Students and residents absorb the values modelled by their mentors “whether these comply with institutional mission statements, goals, and codes of conduct or not.”5 How experienced clinicians manage challenging encounters with patients may be one of the strongest ways that values are transmitted. Regardless of the stated values related to patient-centeredness, trainees can be “exposed to teachers’ negative biases and personal beliefs, including around diverse groups in the community.”5 Careless comments can reveal more about values and priorities than we think: “Offhand ridicule of patients’ weight, poverty, or ethnicity can juxtapose with talk of cultural sensitivity and competence.”2
The hidden curriculum may be sending unintended messages to residents about patients’ “worthiness to receive treatment.”5 In one study, medical students “spoke about how they learned from senior physicians that certain patients, such as those considered to be ‘nice,’ wealthy, or suffering from conditions not resulting from their habits, were more deserving of care than others, such as frequently admitted patients, drug addicts, the elderly, and homeless people.”5 In another, “medical students in Canada were exposed to the concept of a ‘good’ patient as one who prioritized their health and self-care to manage their condition.”5
Using objective and factual terms rather than derogatory ones to describe challenges with patients and barriers to providing care can help trainees see these challenges in the context of clinical decision-making rather than personal biases and frustration with how patients disrupt the efficient delivery of care.5
Residency in O&P should be regarded as a learning experience. While the stated policies of a practice may acknowledge this priority, hidden messages may communicate that productivity is valued more than education. “Tools of evaluation…are not simply instruments of assessment. They also are vehicles for conveying what is and is not important within the organization.”6 Resident evaluations can be a powerful way priorities are communicated. While it is to be expected that residents’ independence, contribution, and productivity increases as their experience grows, describing their value primarily in terms of patient volume and billing can send an unintended message about what really matters. Covering continuing education expenses based on experience and productivity disadvantages novice clinicians, who may benefit the most from additional education.

Revealing the Hidden
“We need to make the hidden curriculum and its messages a topic of explicit discussion and strive to model different messages.”2 The importance of modelling appropriate behavior and attitudes cannot be overstated. When encountering formal instruction about keeping the patients’ needs and goals central and a hidden curriculum of criticism and disrespect, it is not difficult to see which one will have a stronger influence on trainees. Any efforts to teach professionalism will be fatally undermined by persistent patterns of attitude and behavior that contradict stated values. None of us are perfect. Acknowledging our shortcomings when we fail to live up to our highest ideals can reinforce professional standards rather than undermine them. Addressing the hidden curriculum requires a focus on behavioral skills such as “situation awareness, decision-making, communication, and teamwork.”5 Experienced clinicians may need to develop new communication skills, including those related to processing highly emotional encounters with patients and mentoring trainees through difficult situations.
The 2018 American College of Physicians position paper “on the relationship among hidden curricula, ethics, and professionalism” includes principles that can be applied to O&P.7 They recommend group discussions about challenging situations (including “dealing with emotionally difficult patient encounters”) to “better align the hidden and formal curricula.”3,6 Regular check-ins with residents can provide opportunities to discuss any tensions they feel between formal, informal, and hidden instruction and what can be learned from those tensions. Creating safe ways to “acknowledge fears, apprehension, and issues and learn to deal with difficult situations” can improve clinical effectiveness.5
Conclusions
We all have an influence on each other. I’m grateful for the mentors who modelled appropriate professionalism early in my career, the peers with whom I can openly discuss current challenges, and students who have reminded me of the importance of values that can decline in priority over time. Having transparent discussions with students and residents about the hidden curriculum can be a learning opportunity for experienced clinicians. Their perspectives may not be informed by experience, but they can provide a fresh perspective on practices and attitudes that do not affirm our highest values but that we have come to accept as normal.
“One of the greatest challenges facing medical educators today lies in being willing and able to step back and assess just what messages are being created
by and within the very structures they have developed and are responsible for.”6
John T. Brinkmann, MA, CPO/L, FAAOP(D), is an assistant professor at Northwestern University Prosthetics-Orthotics Center. He has over 30
years of experience in patient care and education.
References
1. Association of American Medical Colleges. Medical School Graduation Questionnaire: 2016 All Schools Summary Report. 2016. www.aamc.org/download/464412/data/2016gqallschoolssummaryreport.pdf.
2. Mahood, S. C. 2011. Medical education: Beware the hidden curriculum. Canadian Family Physician 57(9): 983-5.
3. Arora, R., Mukherjee, S. D. 2020. The Hidden Curriculum in Postgraduate Medical Education: A Commentary. Journal of Cancer Education 1-3.
4. https://en.wikipedia.org/wiki/Hidden_curriculum
5. McKenna, L. 2020. Hidden, Informal, and Formal Curricula in Health Professions Education. Clinical Education for the Health Professions: Theory and Practice 1-13.
6. Hafferty, F. W. 1998. Beyond curriculum reform: confronting medicine’s hidden curriculum. Academic Medicine: Journal of the Association of American Medical Colleges 73(4): 403-7.
7. Lehmann, L. S. Snyder Sulmasy, L., Desai, S. 2018. Hidden curricula, ethics, and professionalism: optimizing clinical learning environments in becoming and being a physician: a position paper of the American College of Physicians. Annals of Internal Medicine 168(7): 506-8.
Support authors and subscribe to content
This is premium stuff. Subscribe to read the entire article.


