

The main parameters of normal adult gait are well documented and widely taught in healthcare. For many in the O&P profession, Gait Analysis: Normal & Pathological Function by Jacquelin Perry is a foundational text that introduces the hallmarks of adult ambulation. Similarly, clinicians specializing in pediatric care are familiar with developmental gait, the study of the progression of changes in children’s walking. They have been trained to watch their young patients meet age-appropriate milestones such as walking without assistance, the ability to balance on one leg, and finally achieving heel-to-toe propulsive gait.
Gait analysis in older adults also deserves special attention and requires a nuanced understanding of normal locomotion and the physiological changes associated with aging. Perry’s work provides one benchmark against which deviations are assessed. Generally, normal gait is efficient, energy-conserving, and predictable, whereas geriatric gait reflects adaptive strategies in response to declining physiology, pain, comorbidities, and other challenges.
The Aging Process
In considering geriatric gait, it is important to make clear distinctions. The definition of geriatric can sometimes be arbitrary, simply referring to a person over the age of 65. More specifically, it often refers to frail or vulnerable patients experiencing chronic illnesses or complex health issues. There can be a wide disparity between a patient’s chronological age (the number of years they have lived) and their physiological age (a measure of how well their body functions). Two 75-year-old individuals may demonstrate markedly different gait patterns depending on cardiovascular fitness, neuromuscular integrity, and musculoskeletal health. Physiological age is far more predictive of gait performance, fall risk, and even rehabilitation potential.
Frailty has a clinical definition of age-related physiological decline, characterized by reduced physicality presenting as diminished strength, energy, and physical function. Frail patients often have unintentional weight loss and are at increased risk for falls, hospitalizations, and disability. Their reduction in stamina and overall resilience directly affects their gait.
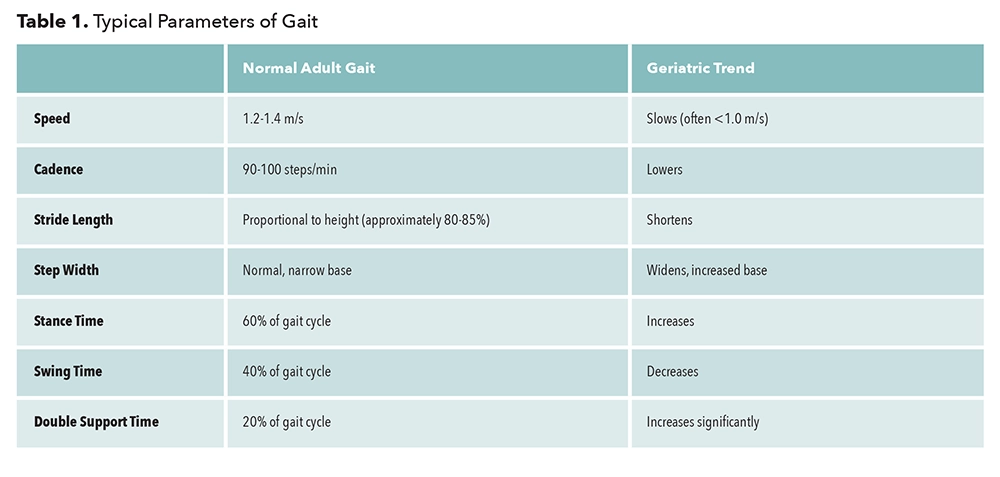
With age there can be obvious changes in joint kinematics, including reduced hip extension in terminal stance, reduced knee flexion during swing, decreased ankle plantarflexion at push-off (pre-swing), and an attenuation in arm swing. Some clinically measurable differences are outlined in Table 1. Many of these adaptations reflect a stability-first strategy, where the patient prioritizes balance over efficiency. A reduction in power at pre-swing contributes significantly to decreased walking speed and increased metabolic cost.
Assessments and Tests
To establish a baseline of gait, clinicians can easily integrate observational gait analysis with standardized tests. The Timed Up and Go Test assesses mobility and fall risk, whereas the 10-Meter Walk Test measures gait speed. The Six-Minute Walk Test evaluates endurance. The Romberg test is a quick and easy way to assess balance, while the Berg Balance Scale is a more comprehensive measure of functional balance. Versions of the Dynamic Gait Index can be employed to assess gait adaptability. It tests the participant’s ability to maintain walking balance while responding to different tasks.
There are also many commercial systems available to measure the kinetic and kinematic variables of gait such as in-shoe pressure mapping and video gait analysis.1 Beyond simply recording metrics, testing serves another purpose by establishing a personal reference for the patient. When a practitioner can demonstrate quantifiable improvements, patients often become more interested in their performance.
Besides biometrics, it is beneficial to note other factors that may contribute to gait deterioration. Foot pain at any age inhibits physical activity, resulting in a sedentary lifestyle. Poorly fitting or unsuitable footwear like clogs, flip-flops, and slippers also limit walking.
Improving Gait in Older Adults
Fortunately, many things can be done to tackle age-related declines in physical function and gait. The best approach is through exercise programs that address strength, flexibility, and endurance. Strength training should focus on lower-limb muscles important for ambulation including the quads, glutes, and plantar-flexors. Maintaining flexibility by stretching the hip flexors, hamstrings, and Achilles tendons is also important as it helps with stride length and posture. With consistent activity, this allows an individual to maintain a level of fitness.
To address the loss of motor skills, programs of task-oriented motor learning have been developed and include balance training and perturbation training. The goal is to sharpen muscle sequencing patterns, timing, and coordination for better walking ability.4 Good examples of this are Tai Chi, which is known to reduce fall risk and improve balance, and traditional yoga, which enhances flexibility and proprioception.5 Structured walking programs can improve endurance, gait technique, and symmetry.
Sagittal Plane Movement
Forward progression of the body depends on sufficient range of motion (ROM) at the major joints; any limits or interruptions in motion directly impact gait efficiency and fluidity. During the physical exam special attention must be given to sagittal plane motion at the hip, knee, and ankle. Many older patients may have had, or be in need of, a hip or knee replacement. Even when the complaint is unilateral, the compensations can be global. Patients in discomfort and pain walk less, walk slower, and lose overall conditioning, weakening both limbs. Once the surgery is complete, physical therapy becomes essential to rehabilitate the patient and address the muscle atrophy and joint stiffness that has developed bilaterally.
Sometimes overlooked, the smooth operation of the first metatarsal phalangeal joint (MPJ) is of immense importance, as it has tremendous influence on gait. During midstance, once heel lift begins, the first MPJ is the sole pivot about which the body mass rotates. Any block in motion at the first MPJ directly affects proximal joint motion. When restricted it can lead to a variety of compensations as the body naturally seeks alternate paths to continue forward. Extensive work by Dananberg outlined the effects of functional hallux limitus on gait.6,7 Some of the main results, reported in a previous article in The O&P EDGE, include orthotic recommendations to raise the medial longitudinal arch, support the midfoot, and maintain the first MPJ in proper sloped alignment.8 Orthotics can be modified in several ways to allow the first metatarsal head to sit lower and improve the operation of the joint. Similarly, a reverse Morton’s extension provides a distal channel that the first metatarsal head and phalanx can sit into.
Orthotic and Pedorthic Recommendations
Given that lower-limb pain is one of many factors that restricts ambulation, foot orthotics can be helpful in encouraging mobility. Custom foot orthotics can be designed to address discomfort and pain in the feet and optimize joint position. Providing medial longitudinal arch support, a deep heel cup, and total plantar contact stimulates sensors on the bottom of the foot. Neutral rearfoot posts provide stability. Pads and depressions may be included to relieve areas of bony prominence or specific pain. Orthotics can also be used to address leg length discrepancies and other asymmetries discovered in a thorough biomechanical exam.
Properly fitting footwear appropriate for the specific environment is essential. Begin by measuring both feet and choosing the best shoe last for the foot type. Footwear for seniors should have some heel elevation, positioning the foot in mild plantarflexion, but no more than 1 inch high. Textured soles and a slight posterior heel bevel can prevent slipping. As proprioception is important to balance and confidence, selecting a high collar shoe, such as a chukka or high top, that activates mechanoreceptors around the malleoli may improve sensory feedback. Likewise, the sole should not be too soft since this overly dampens vibration. A reasonably firm-soled shoe with stiff heel counters and broad flared heels that flex at the ball of the foot is ideal. Clearly, lace or Velcro closures that snug the foot and ankle are better than loose fitting sandals, slippers, clogs, or other styles. Rocker-soled shoes can augment sagittal plane motion restrictions and alleviate the worst consequences of hallux rigidus. However, some patients may find them unstable as they might compromise their balance.
In general, patients should seek routine podiatric footcare. Management of pedal calluses, nail deformities, and other foot problems such as hallux valgus and hammertoes can help keep them pain free and ambulating well into old age. This is especially important if the patient has diabetes and there is any indication of peripheral neuropathy. When appropriate, some patients should be encouraged to use canes, walkers, or other assistive devices. Although they can interfere with the rhythm of the stride, it is better to keep walking, and walk confidently, than risk a catastrophic fall.
Conclusion
Geriatric gait can be seen as a series of compensatory adaptations to a decline in physiology. It is often characterized as slowing down, disrupting the body’s natural dynamic equilibrium and leading to instability. Optimizing gait in older adults requires a multidisciplinary approach, integrating biomechanical insight and clinical assessment. Programs exist to address deficiencies in strength, endurance, and flexibility, which will enhance mobility, independence, and quality of life in seniors. If “exercise is medicine,” and “movement is life,” we as lower-limb specialists have a wonderful opportunity to provide real service to our older patients.
Séamus Kennedy, BEng (Mech), CPed, FAAOP(A), is president and co-owner of Hersco Ortho Labs, New York. He can be contacted at seamus@hersco.com or by visiting hersco.com.
References
- D’Amico, J. 2023. Geriatric gait: Assessment, biomechanics and clinical significance. Podiatry Management 42(7).
- Volpi, E., R. Nazemi, and S. Fujita. 2004. Muscle tissue changes with aging. Current Opinion in Clinical Nutrition and Metabolic Care 7(4):405–10.
- Kennedy, S. 2024. Fall risk and prevention in the elderly. The O&P EDGE 23(11):34-6.
- Brach, J., and J. VanSwearingen. 2013. Interventions to improve walking in older adults. Current Translational Geriatrics and Experimental Gerontology Reports 2(4):10.
- Chen, W., et al. 2023. Tai Chi for fall prevention and balance improvement in older adults: A systematic review and meta-analysis of randomized controlled trials. Frontiers in Public Health 11:1236050.
- Dananberg, H. 1993. Gait style as an etiology to chronic postural pain. Part I functional hallux limitus. JAPMA 83(8):433-41.
- Dananberg, H. 1993. Gait style as an etiology to chronic postural pain. Part II postural compensatory process. JAPMA 83(11):615-24.
- Kennedy, S. 2014. Hallux limitus and the vital operation of the first MPJ. The O&P EDGE 13(5):60-2.



{kind=link}