
A new study in Science Translational Medicine describes three software innovations that substantially improved the user experience and performance of the BrainGate brain computer interface (BCI). Innovations in the decoders now allow the system to recalibrate itself so users can work with BrainGate for longer sessions without interruptions for calibration by technical staff. The team of researchers said the gains are a significant advance in their ongoing work to develop and test a practical BCI assistive technology that people with paralysis could use easily, reliably, independently, and on demand to regain control over external devices.
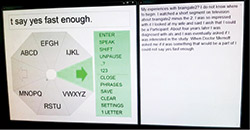
BrainGate2 clinical trial participant T6 used the brain-computer interface to control a specially designed radial keyboard. Innovations in the system’s decoder keep the system calibrated automatically. Photograph courtesy of Braingate.org.
Intracortical BCIs such as BrainGate use a tiny array of implanted electrodes to pick up the electrical activity of neurons in the motor cortex of the brain. Computers then translate those signals into digital commands that have allowed users to control electronic devices such as computers and robotic arms by simply intending to move their own arm or hand. The translation relies on a decoder-an algorithm that infers the movement intentions of the user from the patterns of their neural activity.
A challenge of decoding movement intention from intracortical electrodes is that the signals change over time, causing the performance of the BCI-the ability of users to move a cursor or robot by thinking about the move-to decline until it can be recalibrated. This recalibration is typically performed using a special task in which the participant tries to move the cursor to prescribed targets so that movement intentions can be mapped to the new neural activity patterns.
The essential advance in the new study is a set of decoder upgrades that allows the algorithm to recalibrate itself during practical BCI use without making the user stop for the calibration task every time the signals change. Results of the research reported in the paper show that the new decoder preserved BCI performance much longer than before and even contributed to improving users’ accurate typing speed on an on-screen keyboard.
“Eliminating the need to run a calibration task whenever the recorded signals change will make a clinical BCI more user-friendly and easy to use,” said lead author Beata Jarosiewicz, PhD, assistant professor of research in the Department of Neuroscience at Brown University (Brown) and the Brown Institute for Brain Science, and investigator at the Providence Veterans Affairs Medical Center (PVAMC), Rhode Island.
The BrainGate team includes scientists, engineers, and clinicians from Brown; Massachusetts General Hospital, Boston; PVAMC; Stanford University (Stanford); and Case Western Reserve University.
In a demonstration at the Stanford site of the pilot clinical trial, a woman identified as T6, who was diagnosed with amyotrophic lateral sclerosis, was able to use BrainGate for six sessions of a few hours each over the course of 42 days without any interruptions for explicit recalibration after the decoder was initialized on the first day. T6 was able to type paragraphs, pausing and unpausing the BCI on her own, while the decoder calibrated itself.
The team performed several research sessions to confirm that the new innovations were making a significant and positive difference among the participants. These included asking participants to type for an hour or two in some sessions when the self-calibration innovations were engaged and some when they were turned off. Performance remained stable in sessions when the features were on, but degraded significantly when the features were off. In one of the research sessions with the innovations turned off, the researchers found that turning them back on allowed the system to rescue performance after it had been degrading for lack of the features.
In principle, the improved decoder can be applied to other BCI tasks such as 3D control of a robot arm or even a person’s own electronically reanimated arm or hand. There are unique challenges to doing that, Jarosiewicz acknowledged, but it’s a problem the team is tackling next. The goal remains to develop BrainGate into a system that would be available to people who need it, whenever they need it.
Editor’s note: This story was adapted from materials provided by Brown University.


