
 Partial hand amputation is extremely common. According to the oft-cited Ziegler-Graham study on limb loss prevalence in the United States, amputations of the fingers and hand account for 92 percent of all upper-limb amputations, or approximately half a million cases in 2005.1 Among western countries, the annual incident of partial hand amputation has been estimated at 1 for every 18,000 inhabitants, a ratio that suggests 18,000 new partial hand amputations every year in the United States of 325 million people.2 For many years, the prosthetic options available to this population were limited to aesthetic silicone restorations and less cosmetic but more robust opposition posts. These options have expanded in recent years, a welcome transition that has led to increased interest in the prosthetic management of this historically underserved population. This article reviews recent literature in this area related to upper-limb function, pain, overuse symptoms, and prosthetic options.
Partial hand amputation is extremely common. According to the oft-cited Ziegler-Graham study on limb loss prevalence in the United States, amputations of the fingers and hand account for 92 percent of all upper-limb amputations, or approximately half a million cases in 2005.1 Among western countries, the annual incident of partial hand amputation has been estimated at 1 for every 18,000 inhabitants, a ratio that suggests 18,000 new partial hand amputations every year in the United States of 325 million people.2 For many years, the prosthetic options available to this population were limited to aesthetic silicone restorations and less cosmetic but more robust opposition posts. These options have expanded in recent years, a welcome transition that has led to increased interest in the prosthetic management of this historically underserved population. This article reviews recent literature in this area related to upper-limb function, pain, overuse symptoms, and prosthetic options.
Disability
While most of the literature included in this article has been published in the last few years, a single study from 2004 warrants inclusion as one of the first peer-reviewed manuscripts to specifically report upon a population of individuals with partial hand amputations.3 The study in question examined the extent of upper-limb disability experienced by a convenience sample of individuals with a broad range of diagnoses resulting in upper-limb dysfunction. These included subjects with major unilateral upper-limb amputations, partial hand amputations, complex regional pain syndrome, brachial plexus injury, carpal tunnel syndrome, tendonitis, and arthritis.3 Disability was assessed using the self-report Disability of the Arm, Shoulder and Hand (DASH) survey instrument. The DASH consists of 21 physical activities, inviting subjects to rate the relative difficulty or severity they associate with each task. Higher scores indicate greater disability across this range of activities from writing and food preparation to recreation and transportation. Additional items related to psychosocial function and pain culminate in a 100-point scale with higher levels indicating greater disability.
The greatest levels of disability were reported by those with bilateral upper-limb amputations, complex regional pain syndrome, and brachial plexus injuries, with mean group scores between 65 and 68. By contrast, the mean score for those with major unilateral upper-limb amputations was far less at 39, comparable to the means scores associated with arthritis and carpal tunnel injury. Of relevance to the topic of partial hand amputation, a cohort of 26 individuals with this presentation reported a mean DASH score of 49, significantly higher (i.e., greater disability) than their peers with more proximal amputations.3
The discrepancy between the mean scores of those with major upper-limb amputations (proximal to the wrist) and those with partial hand amputations is not directly addressed by the author. However, she does speculate that “the relatively low scores of patients with a major upper-limb amputation are perhaps a reflection that they are a group of patients who are immediately recognized in healthcare facilities as needing immediate medical and rehabilitation care. They are almost always offered high technology prosthetic equipment.”
 Thus, one possible interpretation of Davidson’s data is that upper-limb prostheses for those with major upper-limb amputations successfully reduced their levels of disability. Whether those with partial hand amputations utilized prostheses, or whether such prostheses improved function for those with partial hand amputations was not reported. Importantly, the manuscript in question was published in 2004, during an era when partial hand prosthetic rehabilitation was confined to silicone restorations and non-articulating opposition posts. Irrespective of the potential explanations, the strongest message from this data is the observation that these minor amputations appear associated with greater levels of disability than more proximal major amputations.
Thus, one possible interpretation of Davidson’s data is that upper-limb prostheses for those with major upper-limb amputations successfully reduced their levels of disability. Whether those with partial hand amputations utilized prostheses, or whether such prostheses improved function for those with partial hand amputations was not reported. Importantly, the manuscript in question was published in 2004, during an era when partial hand prosthetic rehabilitation was confined to silicone restorations and non-articulating opposition posts. Irrespective of the potential explanations, the strongest message from this data is the observation that these minor amputations appear associated with greater levels of disability than more proximal major amputations.
Psychological Well-being
Fourteen years later, as the development of new prosthetic options has elevated the rehabilitation community’s awareness of this population, a related study brings additional understanding to the challenges they face.4 A convenience sample of 309 patients with upper-limb loss completed a battery of self-report instruments examining the constructs of pain interference, perceived activity restriction, post-traumatic stress disorder (PTSD), depression, emotional reaction to their physical condition, and substance abuse inclusive of alcohol, prescription medication, and illicit drug use.4
The sample included 159 subjects with partial hand amputations and 146 subjects with amputations at or proximal to the wrist. The cohorts were reasonably matched with respect to mean age (mid 40s), gender (nearly 70 percent male), and mean age at the time of limb loss (30s). Traumatic amputation etiology was predominant among both groups but more prevalent in those with partial hand amputations (85 percent) than more proximal amputations (69 percent). Among the queried constructs, differences were observed in reported pain interference, PTSD screening, and emotional reaction.4
Pain interference was assessed with a single validated question, “During the past four weeks, how much did pain interfere with your normal work?” Possible answers included 1 (Not at all), 2 (A little bit), 3 (Moderately), 4 (Quite a bit), and 5 (Extremely). For comparative analyses, the authors chose to coalesce responses into those that experienced any level of pain interference (2-5) and those that did not (1). Within this construct, the authors found those with partial hand amputations were more than twice as likely to experience pain interference as their peers with more proximal amputations.4
PTSD screening was performed using the easily accessible, four-item Primary Care PTSD Screen.5 Participants who answer yes to three or more of the following questions are considered to screen positive.
“In your life, have you ever had any experience that was so frightening, horrible, or upsetting that, in the past month, you….”
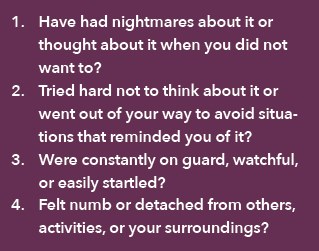
Within this construct, the authors found that nearly one-third of those with partial hand amputations screen-ed positive for PTSD, and that they were nearly twice as likely to do so as their peers with more proximal ampuations.4
The construct of one’s emotional reaction to their physical condition was assessed using a series of questions from the Orthotic Prosthetic Users Survey (OPUS). Sample questions included, “During the past week, how often have you felt easily bothered or upset?” and “…. had difficulty concentrating or paying attention.”4 As with the prior constructs, patients with partial hand amputations reported significantly higher scores on this assessment than their peers with more proximal amputations.4
While statistically significant differences between the two amputation subgroups were confined to those reported above, it is interesting to note that those with partial hand amputations had modest, non-significant higher odds ratios than their peers for likelihood of overuse of prescription drugs, illicit drug use, alcohol use disorder, and positive depression screening. While these odds ratios were small (1.06-1.35), they were consistently higher for those with partial hand amputations.4
In summarizing the impact and implications of their work, the authors conclude, “Overall, these findings suggest that clinicians and occupational therapists should be more cognizant of potential psychological differences associated with their patients’ level of limb loss. More specifically, individuals with partial hand loss may be more susceptible to greater emotional reactions to their loss and increased psychological distress due to the perception of pain interfering with the work and elevated post-traumatic stress. These factors should be considered in the development and throughout implementation of treatment and rehabilitation.”4
Overuse Symptoms
The construct of overuse injury in people with upper-limb loss has been treated before in this publication (“The Prevalence and Impact of Pain Associated with Upper-limb Amputation,” October 2016). However, recent data enables specific consideration of overuse injury among those with partial hand and finger amputations.6
The data in question is derived from a survey in which 82 subjects with partial hand or finger amputations participated. Among these, single-digit amputations were predominant (52 percent), followed by multiple fingers (22 percent), partial hand (14 percent), and thumb amputation (11 percent). Their average age at the time of amputation was 45½ years old, and they reported their experiences at an average of five years after their amputations. Of note, only 7 percent reported using a prosthesis.6
Overuse injuries were reported by roughly one-third of the respondents, a prevalence that mirrors that observed among able-bodied controls and is approximately half that observed among individuals with upper-limb loss at or proximal to the wrist.6 Pain was the predominant symptom (reported by 70 percent of those subjects reporting overuse injury), followed by stiffness (54 percent), tingling (51 percent) and weakness (41 percent).6 The most common location of symptoms was in the affected hand (19 percent), followed by the affected shoulder (13 percent), the non-affected shoulder (10 percent), and the wrist, forearm, and elbow (8-9 percent each).6
Regression analysis was used to identify possible predictors of overuse injury among this population, ultimately identifying residual limb sensations and limited wrist mobility.6 The former may suggest that patients with sensitive residual digits and hand segments are more prone to avoid use of the affected extremity, thereby increasing the functional burden on the sound extremity. The latter may suggest an increased need for proximal joint compensations in the absence of wrist flexion to preposition the residual hand for functional activity.6
Silicone Restoration
While prosthetic restoration for this population has historically been limited to a few options, recent years have seen the development of new components, including body-powered and externally powered systems. While much of the data is pilot level, several recent publications have shed some light on the outcomes facilitated by various prosthetic approaches.
A pair of publications from a research hospital in Slovenia has described the benefit of silicone digit restorations.7-8 Reporting on a population of 42 individuals with single (67 percent), double (21 percent), triple (10 percent), and quadruple (2 percent) partial finger amputations, the articles examine both functional and more holistic variables.
Using the popular Southampton Hand Assessment Procedures (SHAP), grip indices were observed to improve across most grips (e.g., tripod, tip, power, etc.). However, among the tested grips, statistically significant improvements with the prostheses were confined to spherical (as used to hold a ball) and extension (as used to hold a sandwich). However, even these improvements were modest, falling short of the estimated minimum real difference of two points.7
Grip power was assessed for both the power grip and tip prehension. The former realized a non-significant improvement with the use of silicone digit prostheses, while the latter realized a significant decline of approximately 10 percent as prehensile power appeared to be mitigated through the silicone extension worn over the residual digit.7
Thus, it is not surprising to note the findings in a subsequent publication from the same patient cohort observing that the majority of these individuals found that the silicone prostheses were limiting when engaging in vigorous activities such as lifting heavy objects and participating in strenuous sports.8 In contrast, the prostheses were rarely experienced as limiting the social functions of maintaining friendships and visiting friends.8 Among several queried constructs of adjustments and satisfaction, satisfaction with the prostheses was given the highest scores, followed by general adjustment. Of note, the average reported daily use of the silicone prostheses was just over eight hours, with higher daily prostheses use found to correlate positively with general adjustment scores.8
Discussing their observations, the authors remind us that amputation of fingers poses a “triple threat to the quality of life, because it involves loss of function, loss of sensation, and loss of body image.”8 While the silicone prostheses appeared to fall short with regard to dexterity and grip strength in this patient sample, their positive impact on body image was strongly supported.
Externally Powered Solutions
In addition to quantifying the impact of long-existing prosthetic solutions, recent literature has provided a more objective understanding of the impact of externally powered digits among patients with partial hand amputations.9 Specifically, a recent study in the Journal of Prosthetics and Orthotics reported upon the functional impact of Touch Bionics’ i-digit prostheses on the manual function of patients with four-digit (n = 6) and five-digit (n = 9) partial hand absence.
Unlike the silicone prosthesis cohort previously described, for whom minimal changes in the SHAP were observed, among this population with more profound deficits and more elaborate prostheses, the improvements were striking. For those with only their anatomic thumb remaining, average SHAP scores increased from 48 to 67 on the 100-point scale.9 For those with five-digit absence, the results were even more striking, increasing from an average of 13 to 55.9
Further observations were facilitated using the Patient-Specific Functional Scale (PSFS) in which patients identify personal goals and rate their performance ability from 0 (inability) to 10 (able-bodied ability). Again the results were striking, with average increases of 5.4 and 6.8 among the five-digit and four-digit prosthesis users respectively.9 While the items on the PSFS were unique to each individual, there were common tasks within patient portfolios including cutting food, drinking from a bottle, tying shoelaces, opening a bag, and writing. Among this common core of activities, mean increases of 5.6 points on the 10-point scale were reported.9
External Power Versus 3D-Printed Body Power
A final case study reported a single patient’s experience with a Touch Bionics five-finger i-digit externally powered prosthesis and a Raptor Reloaded 3D-printed body-powered prosthesis. Once again, the SHAP was used to facilitate comparison of the two prosthetic solutions.10 Aggregating the index scores for spherical, power, tip, tripod, lateral, and extension grips into an Index of Function score, the patient demonstrated profoundly better function with the i-digit system, realizing an improvement of 50 points compared to the 3D-printed device, as the mean Index of Function scores improved from 25 to 75 on the 100-point scale.10 In a semi-structured interview, the i-digits were rated higher than the 3D-printed solution in the domains of comfort, durability, function, and aesthetics.10 While the inherent limitations of any case comparison should be considered, these differences are striking.
Conclusion
Historically underserved, the population of individuals with upper-limb deficiencies and losses distal to the wrist have become the subjects of increased study as novel prosthetic solutions have become available. While the reviewed articles provide enhanced understanding, additional studies remain needed to refine a collective understanding of the challenges and potential solutions available to this population.
Phil Stevens, MEd, CPO, FAAOP, is in clinical practice with Hanger Clinic, Salt Lake City. He can be contacted at philmstevens@hotmail.com.
Support authors and subscribe to content
This is premium stuff. Subscribe to read the entire article.


